Obliterative Arteriopathy or Graft Vascular Disease(GVD)
Chronic rejection is the single most significant obstacle to long
term organ allograft survival. It similar manifests in all vascularized
solid organ allografts as obliterative arteriopathy or graft vascular
disease(GVD), interstitial fibrosis and atrophy of parenchymal
elements that eventually result in allograft failure. Chronic
rejection usually has an insidious onset, although abrupt arterial
damage from a severe acute rejection can manifest similar arterial
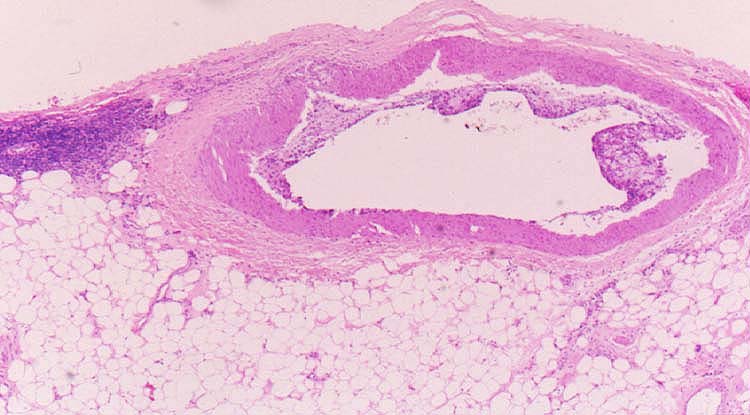
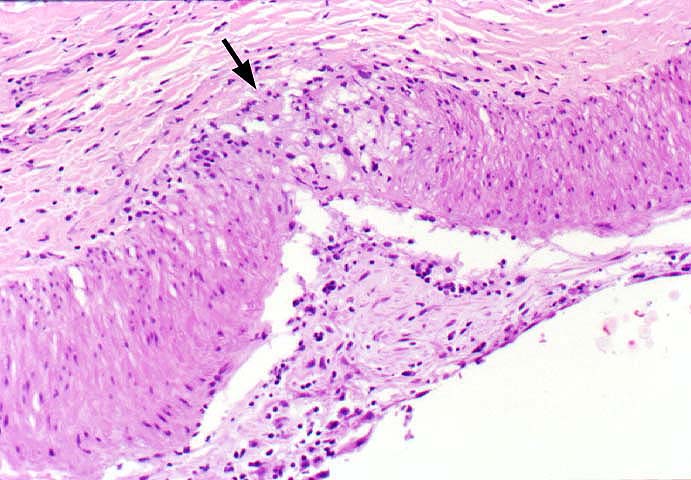
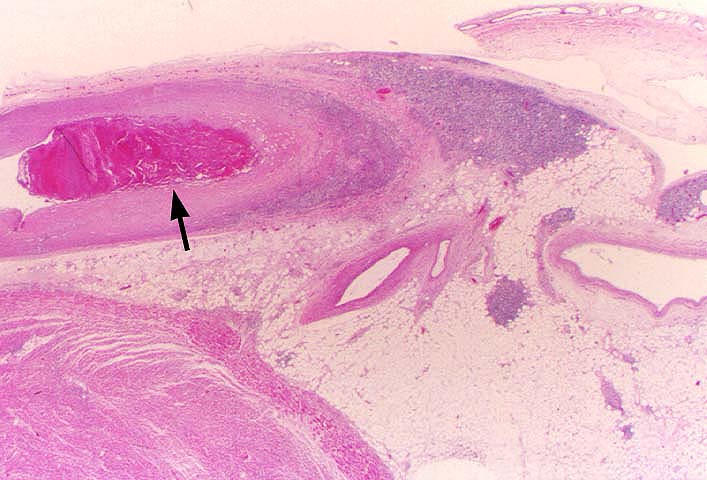
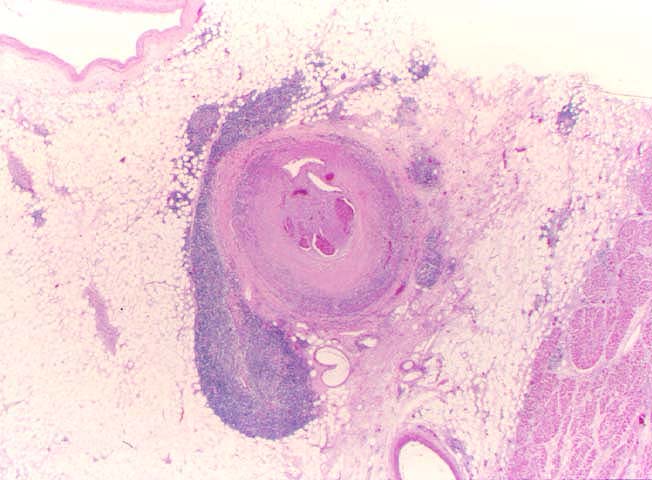
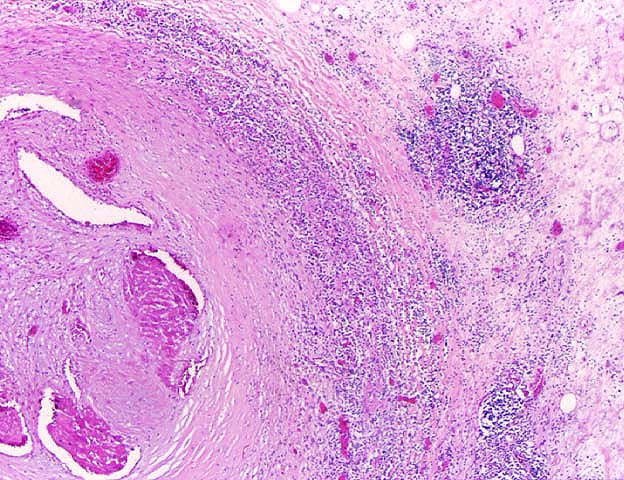
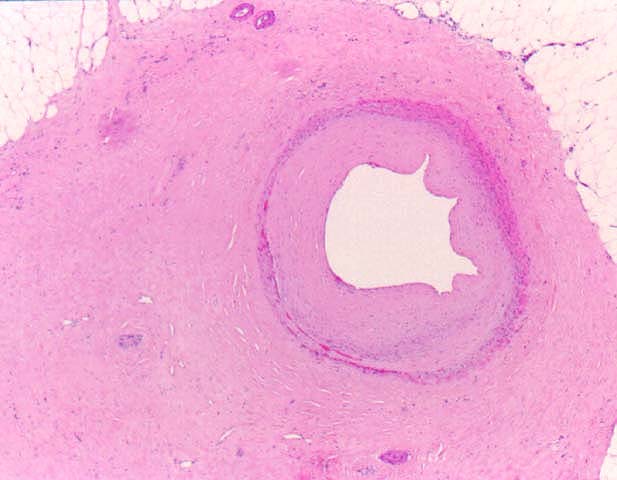
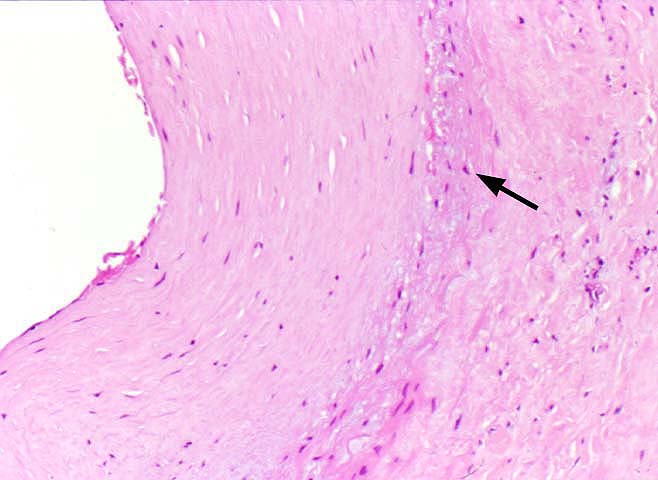
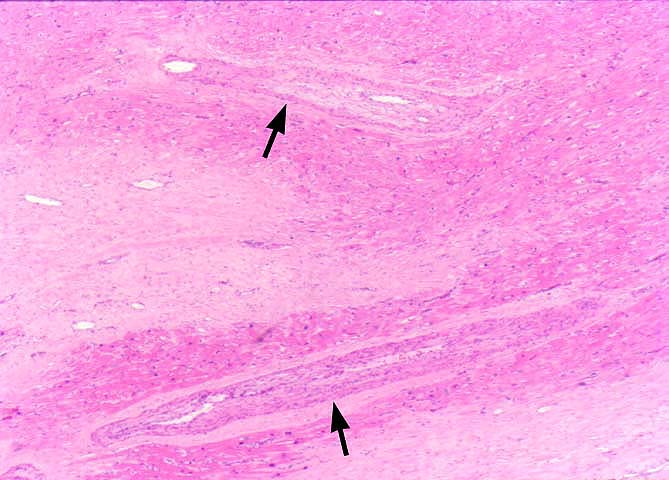
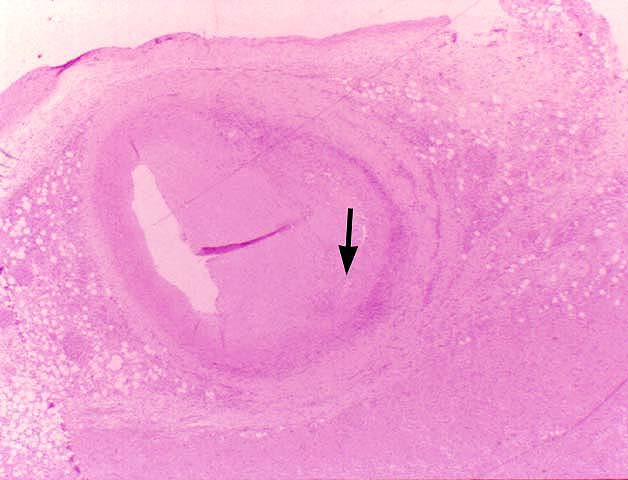
pathology. The principal histopathological finding in GVD is
concentric narrowing of the arterial lumen because of fibrointimal
hyperplasia. Veins are much less frequently and less severely
involved.
Although GVD or OA is similar to atherosclerosis seen in the
general population, there also are distinct differences. A comparison
of the two is shown below:
Table 1. Comparison of GVD and atherosclerosis in
the general population.
Histopathological Finding
Graft
Vascular Disease
Atherosclerosis
Epicardial Coronary arteries
Involved
Preferentially involved
Penetrating intra-myocardial arteries
Involved
Not involved
Endothelium
Often intact, but hypertrophied
Usually intact, hypertrophy not as obvious as GVD
Myointimal proliferation and lumenal narrowing
Yes, concentric
Yes, eccentric
Intimal lipid and cholesterol deposits
Uncommon
Common
Intimal inflammation
Variable
Variable
Elastic lamina
Focally disrupted
Focally disrupted
Media
Thinned in late stage
Thinned in late stage
Medial inflammation
Variable
Variable
Adventitial Inflammation
Common
Variable
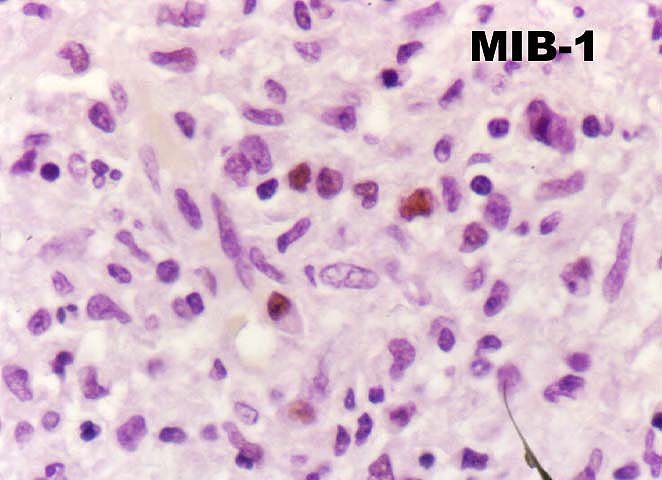
GVD is thought to be due to direct immunological injury to the
allogeneic arterial endothelium, which disrupts intimal homeostasis.
In turn, the injury is thought to trigger a cytokine and growth-factor-driven
arterial repair response that results in lumenal narrowing. Several
excellent reviews of this subject of this subject are suggested
(1-7).
Adams DH, Russell ME, Hancock WW, et al.
Chronic rejection in experimental cardiac transplantation: studies in the
Lewis-F344 model. [Review]. Immunol Rev 1993;134:5-19.
Paul LC, Davidoff A, Benediktsson H. Cardiac allograft atherosclerosis in
the rat. The effect of histocompatibility factors, cyclosporine, and an angiotensin-converting enzyme inhibitor. Transplantation 1994;57(12):1767-1772.