


|
Cytomegalovirus Pancreatitis
The use of newer more potent immunosuppressive drugs such as tacrolimus and mycophenolate mofetil are potentially associated with an increase in all types of infections (bacterial, fungal and viral). Ganciclovir is used prophylactically in many transplant centers to prevent CMV infection. There is evidence that CMV infection is delayed and its severity reduced with ganciclovir prophylaxis.
Although the incidence of CMV disease in kidney-pancreas transplants may be up to 22% in donor positive-recipient negative cases, the actual diagnosis of CMV graft pancreatitis is rare.
In the report of Klassen et al., four patients with CMV pancreatitis diagnosed on percutaneous needle biopsies the process 18 weeks to 44 months after transplantation. In all 4 patients prolonged treatment with ganciclovir achieved clinical and histological resolution of the infection.
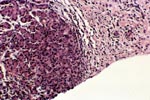
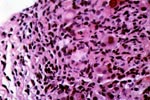
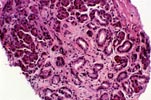
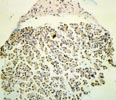
The clinical presentation of CMV graft pancreatitis is indistinguishable from acute rejection, e.g. increase in serum amylase and lipase. Similarly, on percutaneous needle biopsies, acute allograft rejection and mild CMV pancreatitis with scanty viral cytopathic changes show overlapping morphological features. In all cases evidence of viral inclusions should be sought systematically in multiple tissue sections (we routinely evaluate 3 H&E slides and one trichrome stained slide with multiple sections each, immunoperoxidase stains for CMV are performed if deemed necessary).
The inflammatory infiltrates in CMV infection are predominantly lymphocytic and like rejection tend to associate tightly to the acinar parenchyma if this is involved. Some cases show only isolated inclusions in endothelial cells or stromal cells and minimal inflammatory response. Venous endotheliitis is rarely associated with CMV infections. Eosinophils may be rarely seen in CMV pancreatitis as well. Neutrophils are present in association with areas of necrosis or acinar cell damage.
Severe cases of CMV infection may present with intractable gastrointestinal hemorrhage and/or duodenal-cuff perforation.
In summary: Since many features of cellular rejection overlap with CMV graft pancreatitis, the latter infection should always be ruled out with thorough examination of the tissue available, and special stains if necessary, before the diagnosis of rejection is rendered.

Please mail comments, corrections or suggestions to the TPIS administration at the UPMC.
If you have more questions, you can always email TPIS Administration. |
|