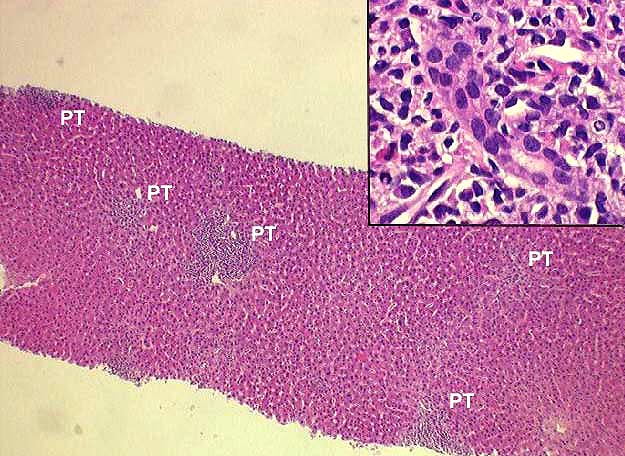
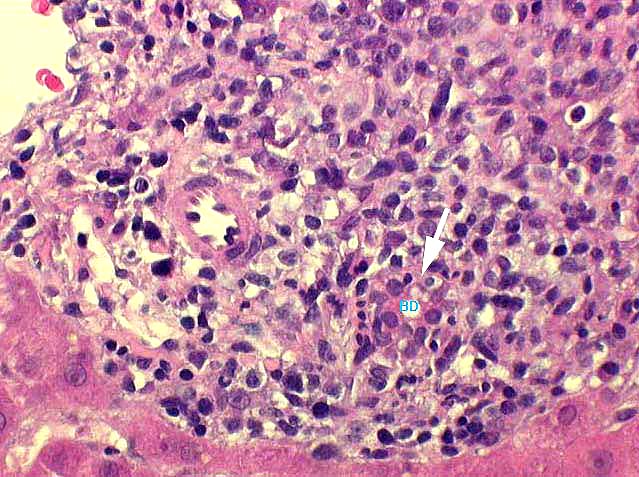
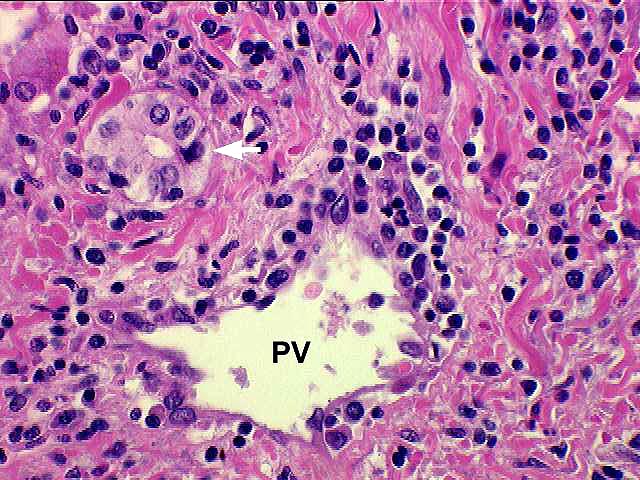
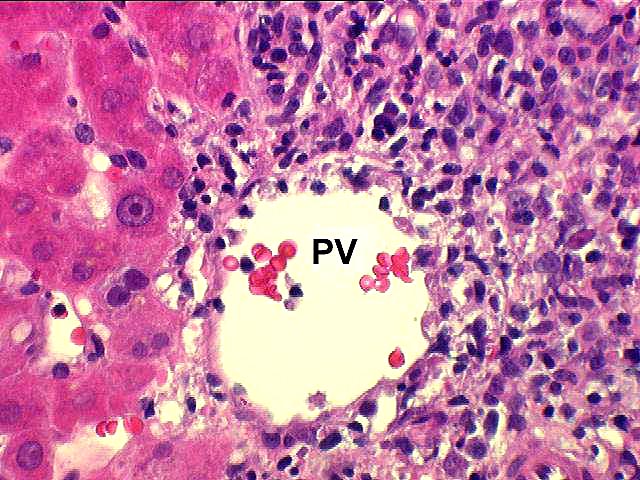
Histopathologically, mild acute rejection is characterized by a "rejection-type" inflammatory infiltrate in a minority of the triads, that is generally mild, and confined within the portal spaces. For those of you who are familiar with liver allograft biopsies, the term "rejection-type" infiltrate will immediately bring to mind, a characteristic histopathological image. For those of who are not familiar with liver allograft rejection histopathology, a typical "rejection infiltrate" consists of blastic(activated) lymphocytes, small lymphocytes, macrophages and fewer neutrophils and eosinophils. However, on occasion, the eosinophilic component can be quite prominent, simulating an allergic drug reaction.
Once a verbal descriptor for acute rejection has been applied, the biopsy is then numerically scored according to the Rejection Activity Index(RAI) outlined in the Banff Schema. Most biopsies graded as "mild" will have total RAI scores of between 3 and 5.
Fortunately, the vast majority of mild acute rejection episodes respond to treatment with increased immunosuppression, either in the form of increased baseline immunousuprression, or pulsed corticosteroid treatment.
REFERENCES
|
|
|
|