Revision of the 1996 Working Formulation for the Standardization
of Nomenclature in the Diagnosis of Lung Rejection
C. CHRONIC AIRWAY REJECTION - OBLITERATIVE BRONCHIOLITIS OBLITERANS
Obliterative bronchiolitis describes dense eosinophilic
hyaline fibrosis in the sub-mucosa of membranous and
respiratory bronchioles, resulting in partial or complete
luminal occlusion (Figures 20, 21, 22, 23 and 24). This
tissue can be concentric or eccentric and may be associated
with fragmentation and destruction of the smooth
muscle and elastica of the airway wall. It may extend into
the peri-bronchiolar interstitium. Mucostasis and/or foamy
histiocytes in the distal air spaces are commonly associated
with obliterative bronchiolitis and may be observed
in transbronchial biopsies in the absence of bronchiolar
occlusion or any bronchiolar tissue.
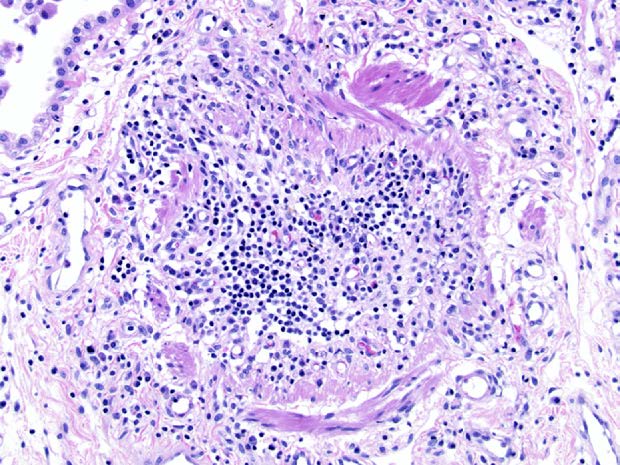
Figure 20. Obliterative bronchiolitis. In this example of obliterative
bronchiolitis, the entire airway lumen has been obliterated by scar tissue
and mononuclear cells, with the circumference of the small airways
defined by an interrupted layer of smooth muscle bundles. H&E.
Figure 21.Obliterative bronchiolitis. This small bronchiole shows
eccentric scarring of the submucosa of the small airway associated
with an inconspicuous peribronchiolar mononuclear infiltrate. The
overlying epithelium appears attenuated, while the lumen of the airway
is distorted. Such partial occlusion of the small airways may be
responsible for significant increases in airflow resistance. H&E.
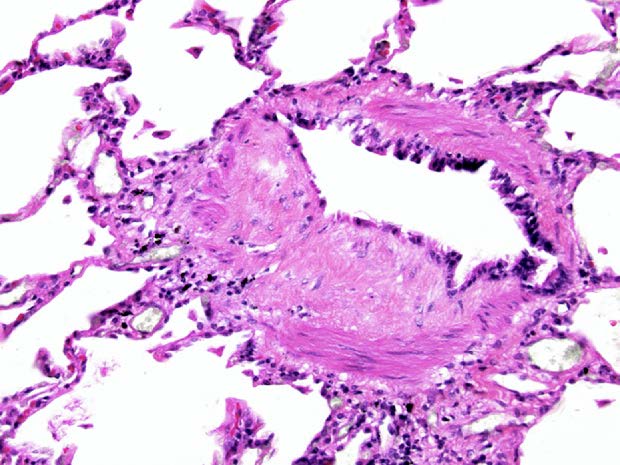
Figure 22.Obliterative bronchiolitis. In this transbronchial biopsy, an
eccentric polypoid plaque of dense eosinophilic scar tissue is superimposed
between attenuated respiratory epithelium and the smooth
muscle wall of the airway. Such focal scarring of the airways is
classified as obliterative bronchiolitis. H&E.
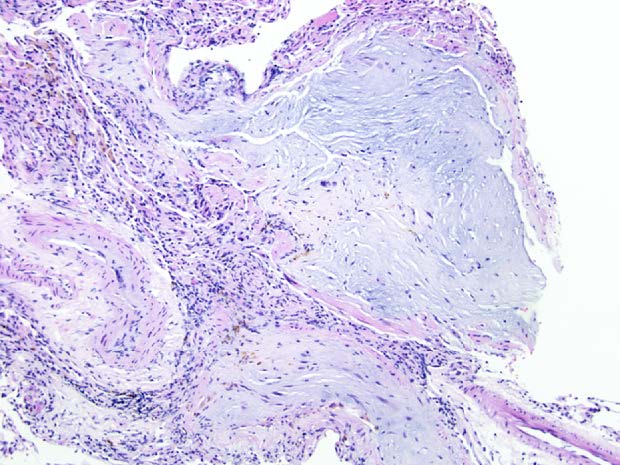
Figure 23.Obliterative bronchiolitis. In this distorted transbronchial
biopsy, the scar tissue which is obliterating the airways has a loose myxoid
quality but still shows dense lamellae of irreversible fibrous scar tissue in
the airways. Once again the location of these scars adjacent to pulmonary
arteries and the residual smooth muscle within the walls of these airways
alert the pathologist to small airway disease. H&E.
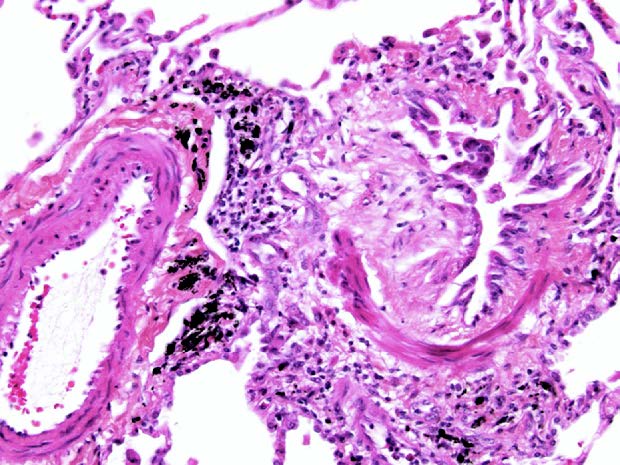
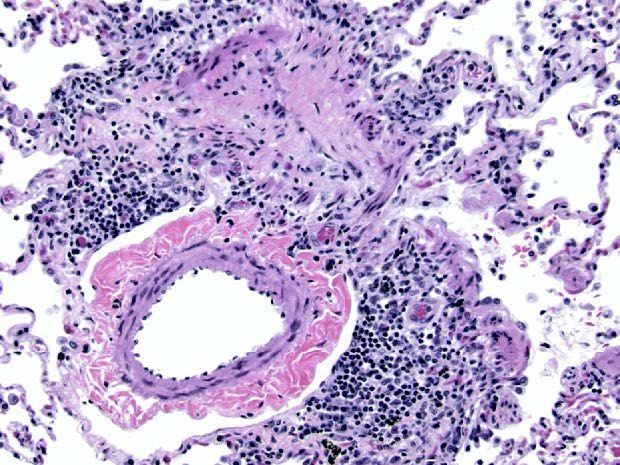
Figure 24.Obliterative bronchiolitis. The hint to underlying obliterative
bronchiolitis in this case is the interrupted cords of smooth muscle
forming a tubular structure associated with dense scar tissue in a
position adjacent to a pulmonary artery. H&E.
The 1996 working formulation concluded that the
1990 distinction between sub-total and total forms of
obliterative bronchiolitis was not useful, but retained
the designation of active vs inactive, depending on the
presence and degree of accompanying inflammation.2
The consensus in 2006 was that the distinction between
active and inactive obliterative bronchiolitis is no
longer useful and the condition should be designated
merely as C0, indicating a biopsy with no evidence of
obliterative bronchiolitis, and C1, indicating that obliterative
bronchiolitis is present in the biopsy. Transbronchial
biopsy is an insensitive method for detecting
obliterative bronchiolitis and the clinical use of bronchiolitis obliterans syndrome (BOS)
with its functional
grading is the preferred means of diagnosing and monitoring
chronic airway rejection.14
Please mail comments, corrections or suggestions to the
TPIS administration at the UPMC.