Revision of the 1996 Working Formulation for the Standardization
of Nomenclature in the Diagnosis of Lung Rejection
B: AIRWAY INFLAMMATION: LYMPHOCYTIC BRONCHIOLITIS
The 1996 working formulation allowed airway inflammation
to be graded from B0 (no inflammation) to B4 (severe airway inflammation).2 The earlier 1990 formulation
recommended airway inflammation co-existent
with Grade A acute rejection to be recorded as present
or absent, but did not reflect the intensity of the
inflammatory infiltrates.1 The 1996 grading of airway
inflammation was not accepted by all members of the
lung rejection study group for several reasons, including
the lack of convincing evidence that airway inflammation
could be used solely to grade rejection because
of its frequent co-existence with airway infection. Also,
there are frequent problems with adequate sampling of
small airways in transbronchial biopsies and with technical
issues such as tangential cutting, etc. An ungradeable
category was designated for those biopsies limited
by sampling problems, infection, tangential cutting, etc.
It was accepted that the scientific and clinical usefulness
of airway inflammation grades would need revisiting
over the course of time.12 However, the format of
Grades A and B in the 1996 classification emphasized
the need to retain perivascular infiltrates as the primary focus in the histologic classification of acute lung
rejection.
At the 2006 consensus meeting, the majority of
pathologists felt that the criteria for separating four
grades of airway inflammation were poorly defined and
difficult to discriminate on transbronchial biopsy. Previous
studies of reproducibility of the 1996 working
formulation both in terms of inter- and intra-observer
variability had shown significant problems with the
airway inflammation B grades in comparison to the
acute rejection A grades and it was recognized that new
recommendations must improve reproducibility.3,4,13
The revision of the B grades has collapsed the four
previous grades into two and retained B0 (no airway
inflammation) and BX (ungradeable for reasons just
stated). The B grade designation applies only to small
airways, that is, bronchioles, and the description of
inflammation in cartilage-containing large airways is
covered later. It is recognized that airway inflammation
can be present in the absence of perivascular infiltrates
and that rigorous exclusion of infection is necessary
before ascribing the features to acute rejection of the
airway.
GRADE B0 (No Airway Inflammation)
In Grade B0 there is no evidence of bronchiolar inflammation.
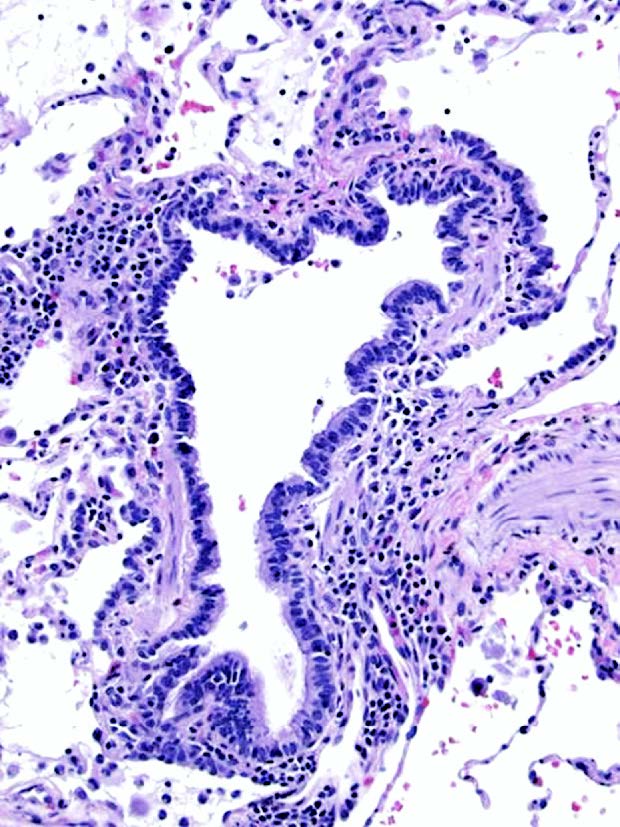
Figure 15. Low grade lymphocytic bronchiolitis (B1R). In this
example the bronchiole shows a mild patchy peribronchiolar
mononuclear cell infiltrate which spares the respiratory epithelium
and is unassociated with epithelial injury. The infiltrate forms an
incomplete circumferential band in places. There is no evidence of
fibrosis in lymphocytic bronchiolitis in comparison with obliterative
bronchiolitis. H&E.
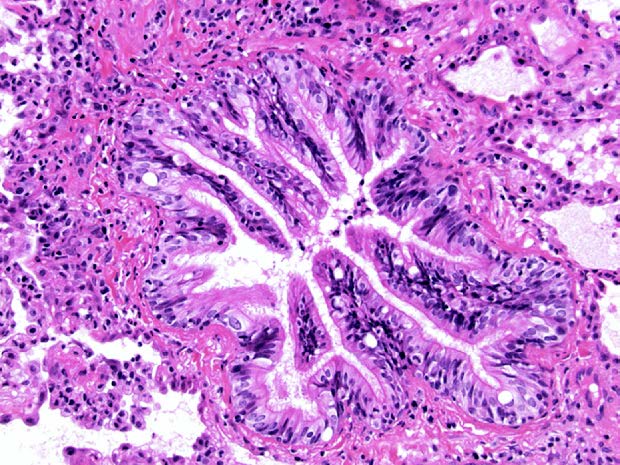
Figure 16. Low grade lymphocytic bronchiolitis (B1R). This terminal
bronchiole shows epithelial hyperplasia and some epithelial undulation
but is accompanied by a very sparse mononuclear inflammatory
infiltrate which does not home to the basement membrane or injure the
mucosal epithelium. H&E.
GRADE B1R (Low-grade Small Airway Inflammation)
In Grade B1R there are mononuclear cells within the
sub-mucosa of the bronchioles, which can be infrequent
and scattered or forming a circumferential band
(Figures 15 and 16). Occasional eosinophils may be seen within the sub-mucosa. There is no evidence,
however, of epithelial damage or intra-epithelial lymphocytic
infiltration. This grade combines and replaces
the previous B1 and B2 grades.
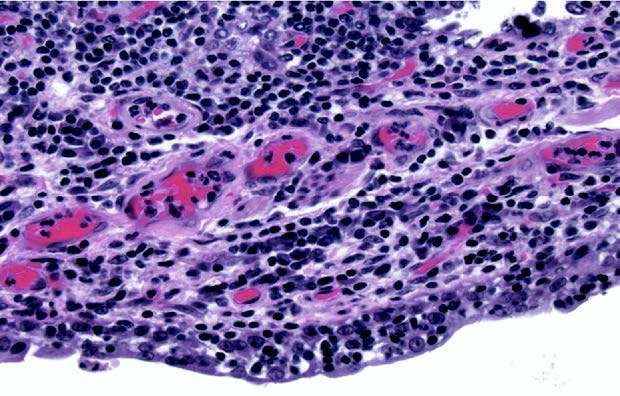
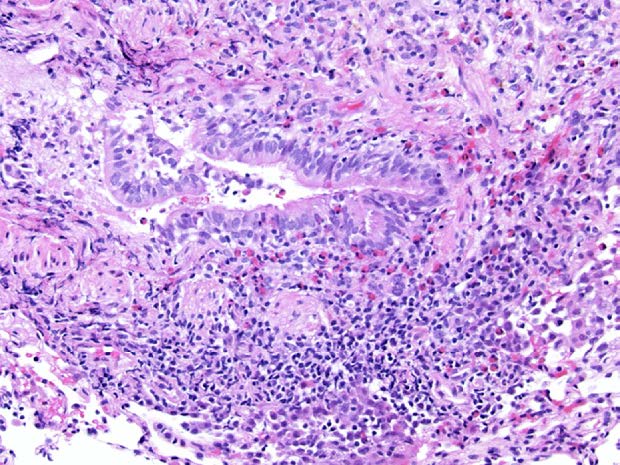
Figure 17. High grade lymphocytic bronchiolitis (B2R). In high grade
lymphocytic bronchiolitis, in contrast to the low grade variant, mononuclear
cells expand the submucosa and home to the epithelial
basement membrane where they percolate through the basement
membrane into the overlying respiratory epithelium. Epithelial cell
necrosis and apoptosis is observed. H&E.
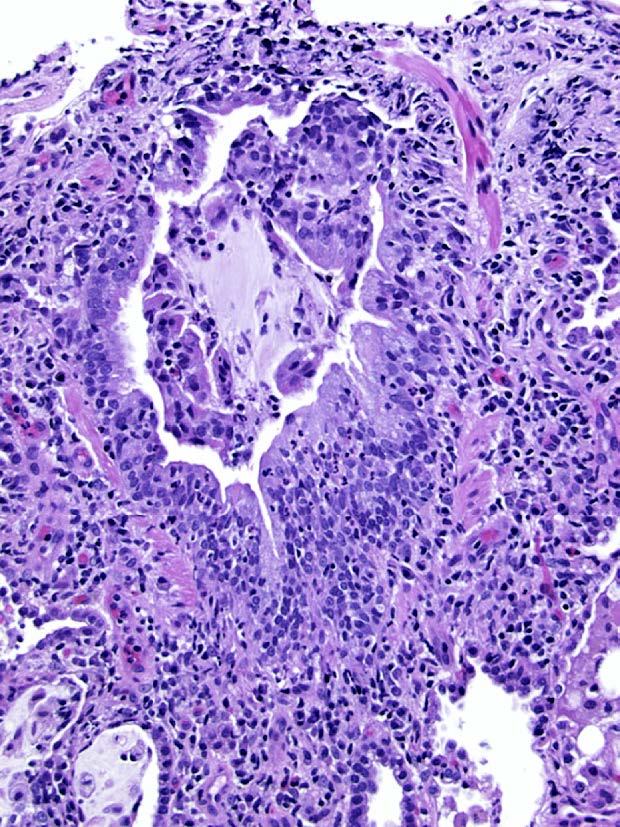
Figure 18. High grade lymphocytic bronchiolitis (B2R). This small
bronchiole shows an intense mucosal and peribronchiolar mononuclear
cell inflammatory infiltrate involving the epithelium with focal epithelial
damage. Neutrophils are present in the epithelium and should not be
confused with infectious bronchiolitis if correlation with microbiology is
undertaken. H&E.
Figure 19. High grade lymphocytic bronchiolitis (B2R). In this example
of a small bronchiole in a transbronchial biopsy, the mononuclear
inflammatory cell infiltrate is accompanied by an intense eosinophilic
infiltrate with eosinophils and lymphocytes traversing the epithelium
accompanied by epithelial cell necrosis. Infection should be excluded
as a cause of the eosinophilia. H&E.
GRADE B2R (High-grade Small Airway Inflammation)
In Grade B2R the mononuclear cells in the sub-mucosa
appear larger and activated, with greater numbers of
eosinophils and plasmacytoid cells (Figures 17, 18 and
19). In addition, there is evidence of epithelial damage
in the form of necrosis and metaplasia and marked
intra-epithelial lymphocytic infiltration. In its most severe
form, high-grade airway inflammation is associated
with epithelial ulceration, fibrino-purulent exudate, cellular
debris and neutrophils. The presence of a disproportionate
number of neutrophils within the epithelium
and sub-mucosa in relation to the numbers of
sub-mucosal mononuclear cells is highly suggestive of
infection rather than rejection. Any accompanying lavage
or aspirate may also be purulent and/or show
evidence of organisms.
GRADE BX (Ungradeable Small Airway Inflammation)
In Grade BX the changes are ungradeable due to sampling
problems, infection, tangential cutting, artifact, etc.
The consensus group recommended that the diagnosis
of acute rejection with co-existent airway inflammation
be in the same form as the 1996 formulation-that
is, acute rejection grade with airway inflammation
grade. For example, moderate acute cellular rejection in
which there is intense small airways inflammation
would be designated moderate acute rejection, Grade
A3, with airways inflammation being Grade B2R. The
category of lymphocytic bronchiolitis is graded as A0,
B1R or A0, with B2R depending on the severity of the
airway inflammation.
Please mail comments, corrections or suggestions to the
TPIS administration at the UPMC.