Previous Biopsies on this Patient:
TPIS Related Resources:
Liver
Allograft Rejection Grading
Liver
Transplant Topics
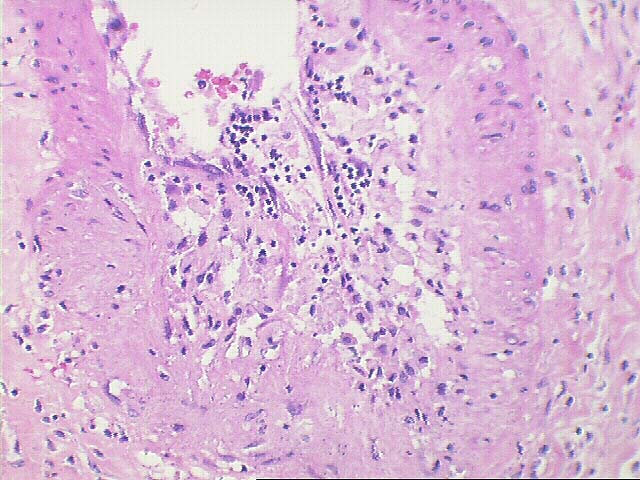
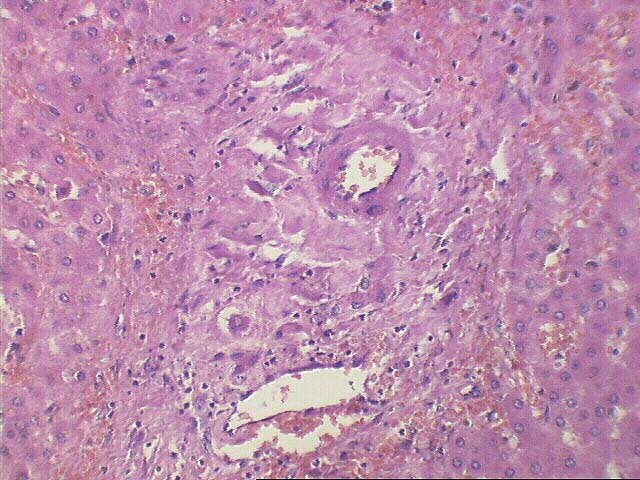
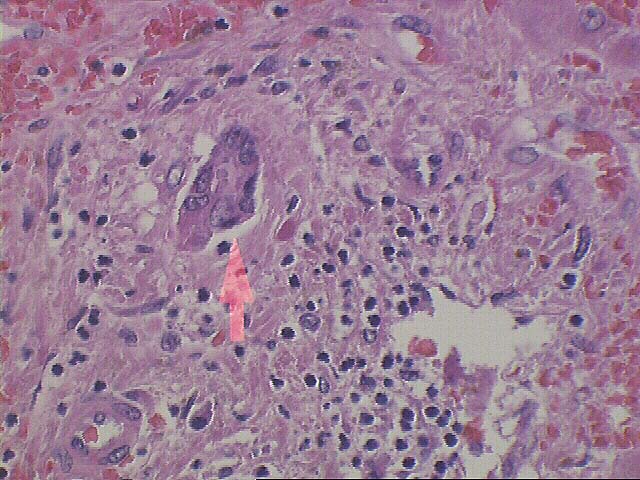
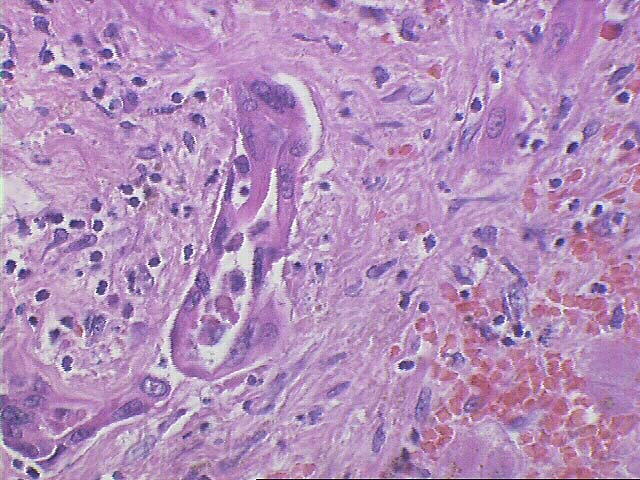
Sections through the hilum of the liver reveal large areas of fibrosis in the hilar connective tissue and mild mononuclear inflammation. There is also perineural edema and depletion and scarring of a hilar lymph node. In addition, there is focal foam cell obliterative arteriopathy and a superimposed lymphocytic arterial intimal inflammatory cell infiltrate, with marked endothelial cell hypertrophy(activation) and focal degeneration of medial myocytes. A small cuff of smaller adventitial macrophages are also seen in the affected vessels.
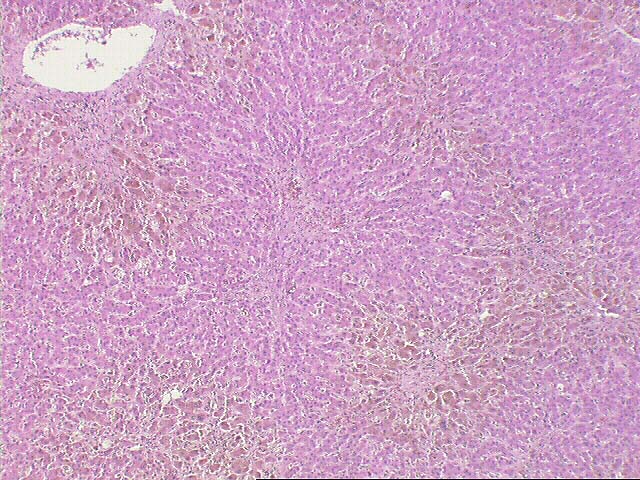
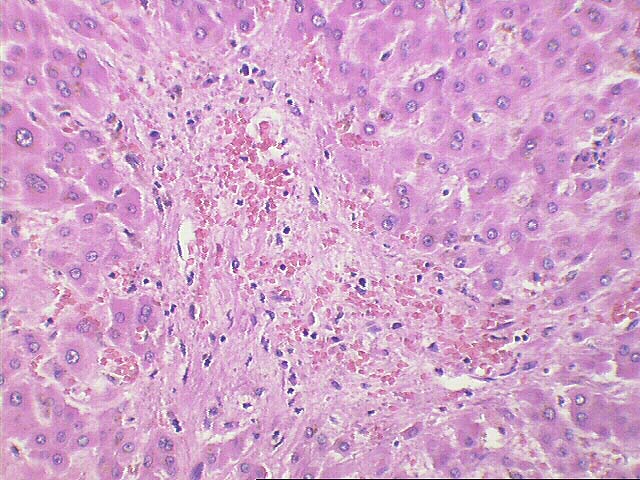
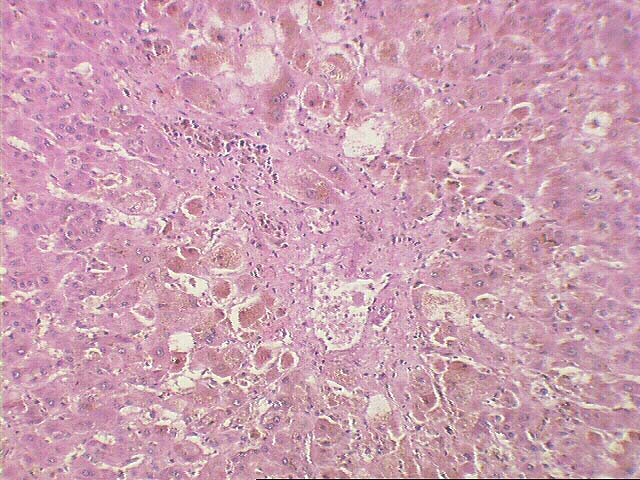
Throughout the parenchyma, the normal lobular architecture is slightly distorted because of mild portal expansion and areas of perivenular hepatocyte dropout, centrilobular congestion and hemorrhage. Loss of small bile ducts variably affects from about 30% to 60% of a random sampling of portal triads. In addition, there is marked eosinophilic transformation, uneven spacing and nuclear enlargement in the remaining ductal epithelial cells and collagenization of the portal tract connective tissue.
There is also marked centrilobular hepatocellular swelling, hepatocanalicular cholestasis, venular endothelial hypertrophy and moderate perivenular fibrosis. Intralobular foam cell clusters are also seen. No definite ground glass cells are detected, but special stains for Hepatitis B core and surface antigens should be used to exclude recurrent infection.
Overall, the histopathological changes are consistent with chronic liver allograft rejection, which appears to have evolved from acute rejection. This contention is based on the obliterative arteriopathy, the active lymphocytic intimal inflammation and the bile duct loss and atrophy.
This page and its contents are Copyright © 1996, 1997 University of Pittsburgh. All rights reserved. Unauthorized redistribution prohibited.