)
)
)
)
)
)
)
)
Severe Acute Rejection
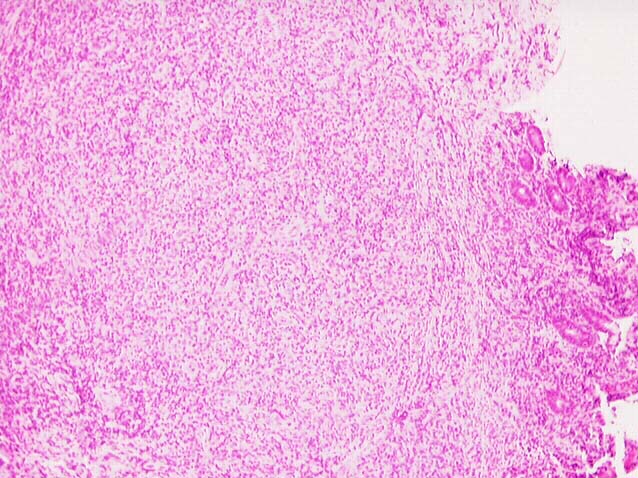
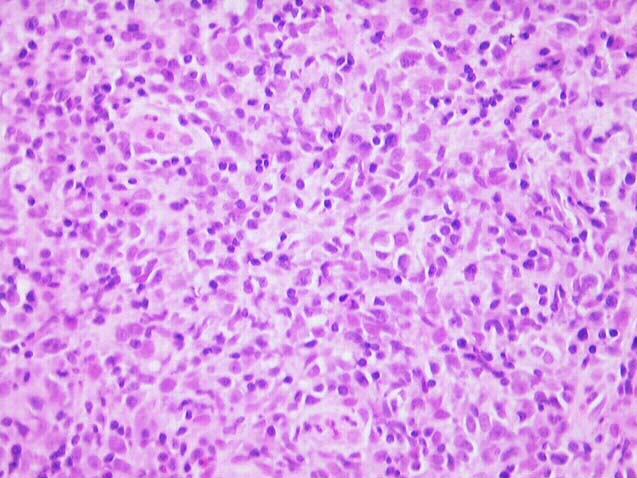
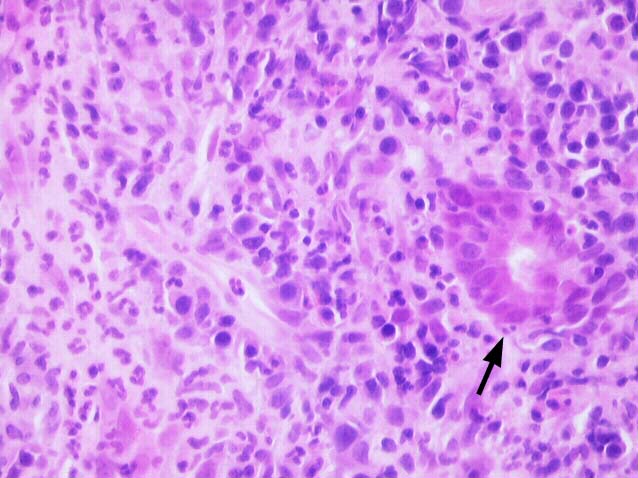
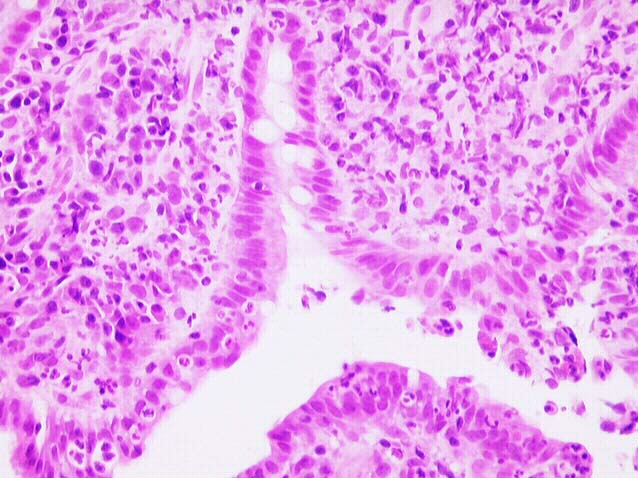
Severe acute rejection is distinguished by a marked degree of crypt damage and mucosal ulceration, with lymphocytic infiltrate extending deep in the allograft wall and involving nerves and ganglia. As a consequence of the mucosal destruction, luminal contents gain access to the submucosa, prompting a neutrophil-rich infiltrate and an overlying fibropurulent (pseudomembranous) exudate with widespread mucosal sloughing as the final result. The adjacent viable epithelium usually shows rejection-associated changes such as crypt epithelial damage and abundant apoptosis. Severe intimal arteritis or transmural arteritits may be seen.
If biopsies are obtained from the necrotic or ulcerated regions or areas with only active inflammation, the deeper rejection-associated changes may not be present in the specimen. Under these circumstance, the overall context and clinical findings then need to be taken into account.
|
|
|
|