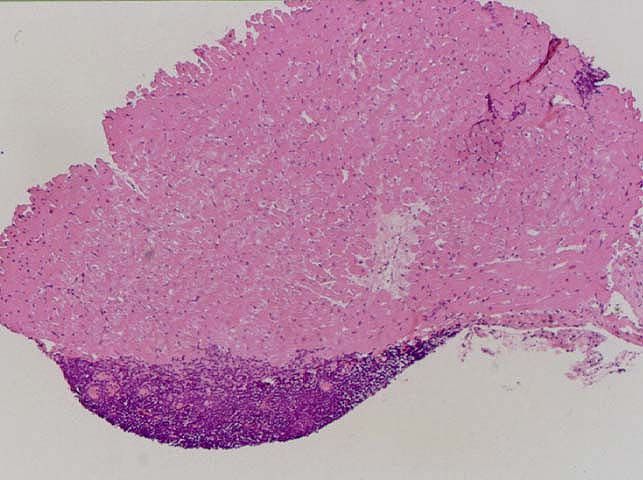
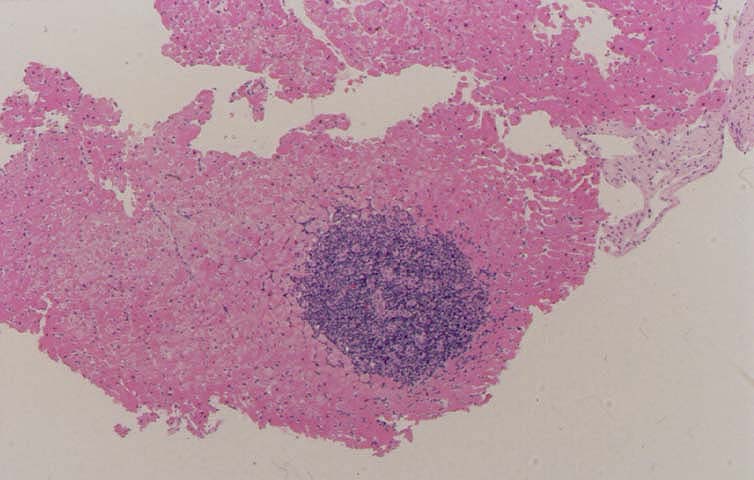
Quilty lesions, also known as endocardial infiltrates,
were first described by Billingham who gave them the surname
of the patient first showing this lesion (1). Quilty lesions have
been the subject of more than a dozen different studies, and
there is still no consensus as to their etiology or significance.
They have been associated with the use of cyclosporine and
waxing and waning levels of immunosuppression (2-4). It has
also been suggested that Quilty lesions represent a "benign"
form of rejection (5), an analogue of vascular rejection (6, 7)
or even incipient post-transplant lymphoproliferative disorder,
the latter of which has been proven incorrect (8). More recent
studies in experimental animals suggest that they may be sites of
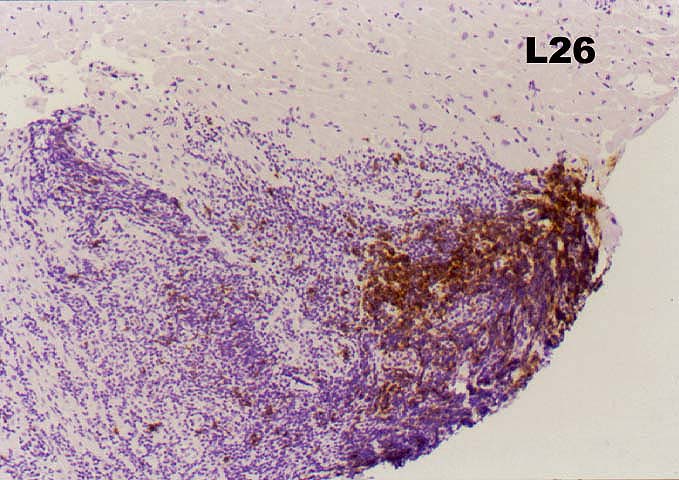
antigen processing and low grade immune stimulation (9). In
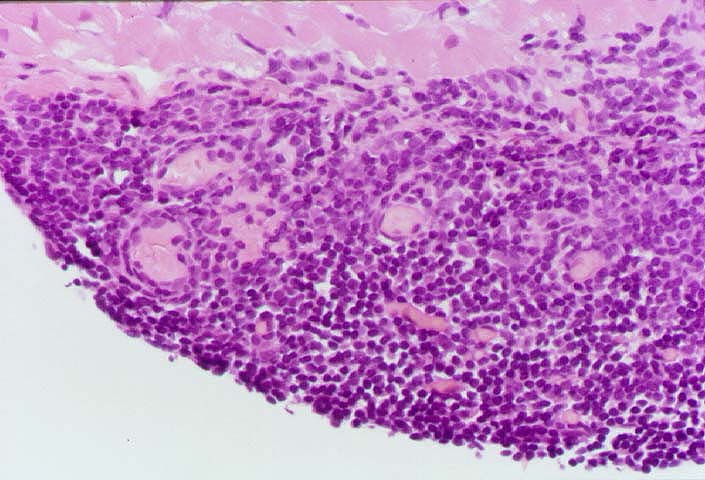
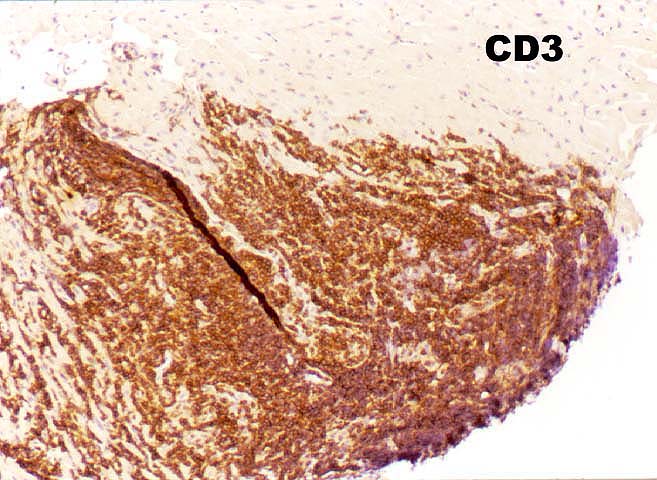
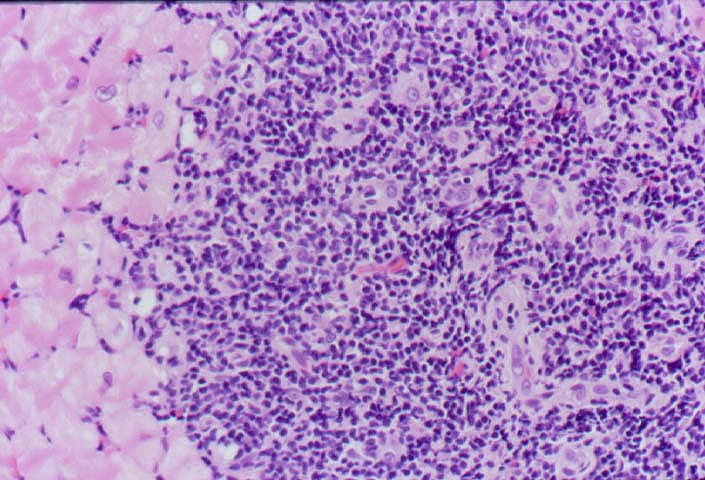
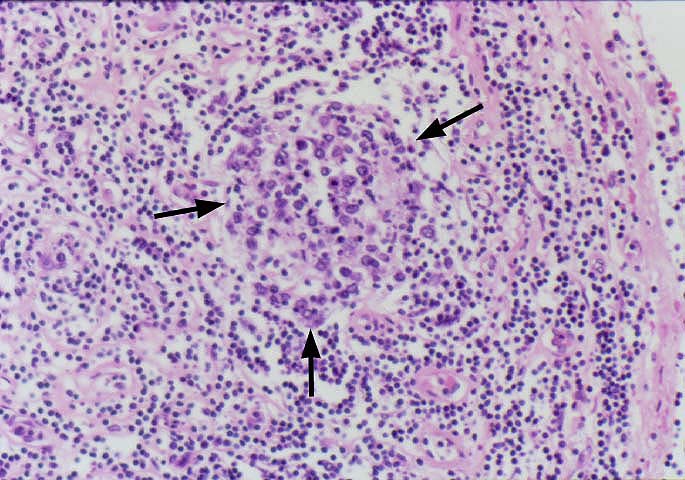
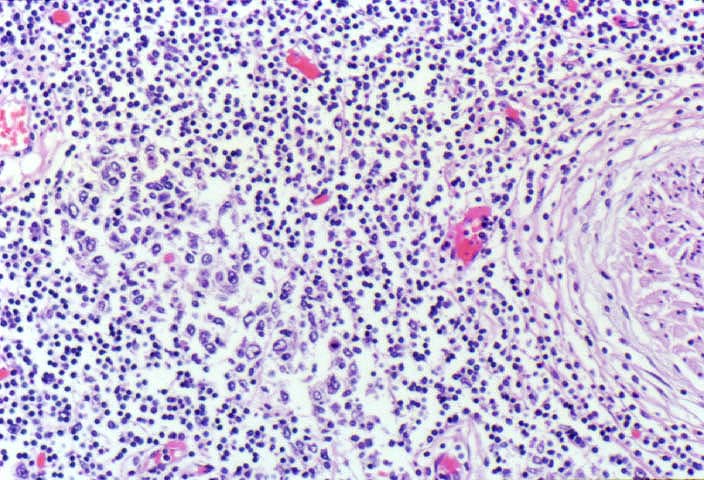
human and experimental animals, Quilty lesion are comprised
predominantly of T cells, with the CD4 subset predominating
over CD8 cells by a ratio of 2-3:1.
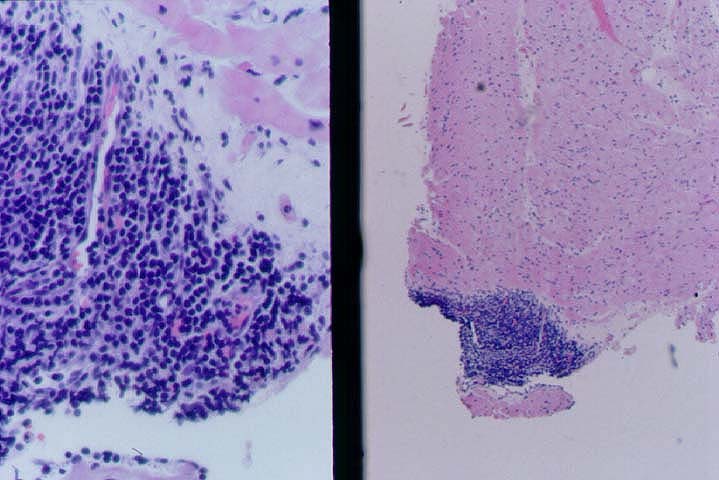
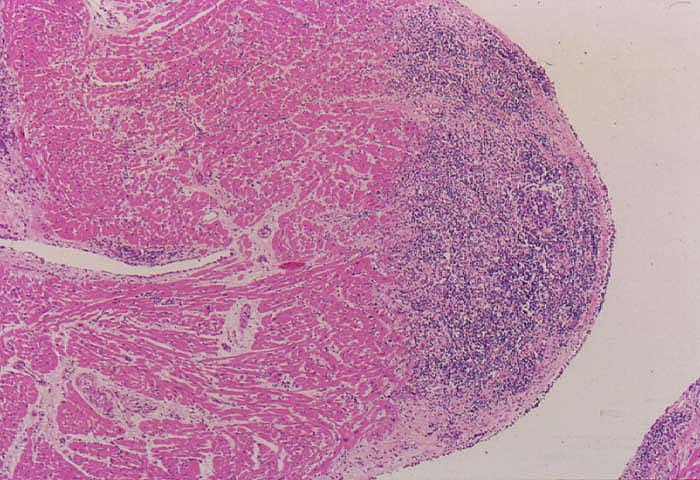
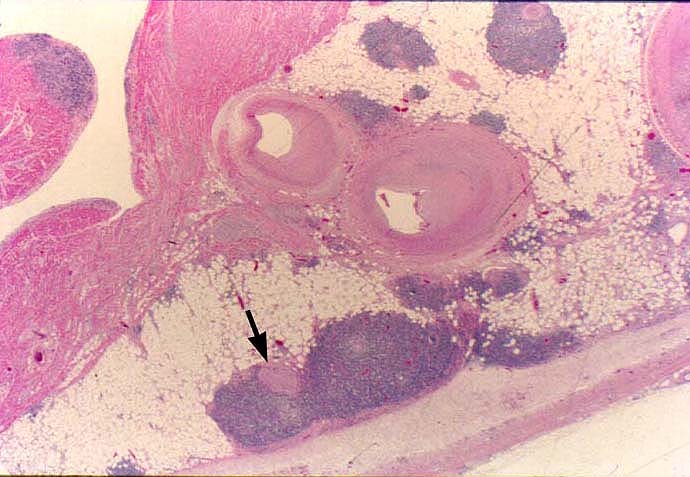
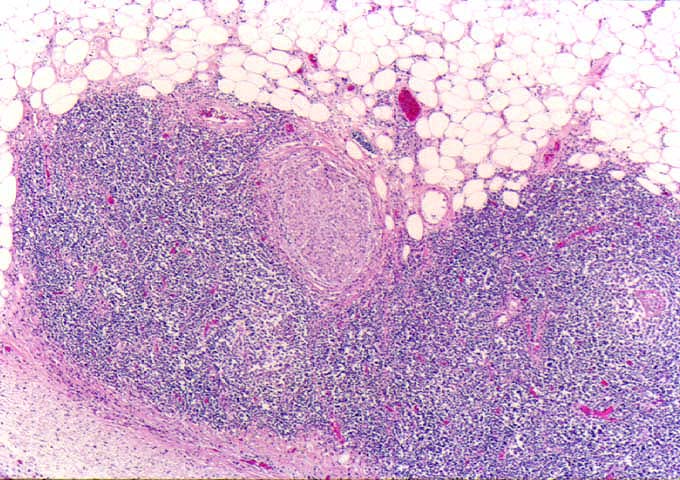
Quilty lesion have been subclassified on the basis of
whether they infiltrate the underlying myocardium. In type A
lesions, the border with the underlying myocardium is smooth.
In type B lesions, the mononuclear cells infiltrate between
myocytes in the underlying myocardium, but myocyte necrosis is
not seen. On a practical level, Quilty lesions are generally not
considered in the grading of cardiac allograft rejection, but
mentioned in the diagnosis as a separate finding.
References
- Billingham ME. Cardiac Transplantation. In: Sale GE, ed. The Pathology of Organ Transplantation. Boston: Butterworths, 1990:133-152.
- Costanzo-Nordin MR, Winters GL, Fisher SG, et al. Endocardial infiltrates in the transplanted heart: clinical significance emerging from the analysis of 5026 endomyocardial biopsy specimens. J Heart Lung Transplant 1993;12(5):741-747.
- Suit PF, Kottke-Marchant K, Ratliff NB, et al. Comparison of whole-blood cyclosporine levels and the frequency of endomyocardial lymphocytic infiltrates (the quilty lesion) in cardiac transplantation.
Transplantation 1989;48(4):618-621.
- Forbes RDC, Rowan RA, Billingham ME. Endocardial infiltrates in human heart
transplants: a serial biopsy analysis comparing four immunosuppression protocols. Hum Pathol 1990;21(8):850-855.
- Joshi A, Masek MA, Brown BW Jr, et al. "Quilty" revisted: a 10-year perspective. Hum Pathol 1995;26(5):547-557.
- Kemnitz J, Cremer J, Schaefers H, et al. Some aspects of changed histopathologic appearance of acute rejection in cardiac allografts after prophylactic application of OKT3. J Heart Lung Transplant 1991;10(3):366-372.
- Kemnitz J. Histopathologic diagnosis of different forms of chronic rejection
in biopsy material from heart allograft recipients. In: Kemnitz J, ed.
Diagnosis of rejection in biopsy material of cardiac allografts:
histopathology and immunopathology. Germany: Wolfgang-Pabst-Verlag, 1991:52-71.
- Nakhleh RE, Copenhaver CM, Werdin K, et al.
Lack of evidence for involvement of Epstein-Barr virus in the development of the
"quilty" lesion of transplanted hearts: an in situ hybridization study.
J Heart Lung Transplant 1991;10(4):504-507.
- Demetris AJ, Murase N, Ye Q, et al. Analysis of Chronic Rejection and Obliterative Arteriopathy.
Possible contributions of donor antigen presenting cells and
lymphatic disruption. Amer J Pathol 1997;150(2):563-578.