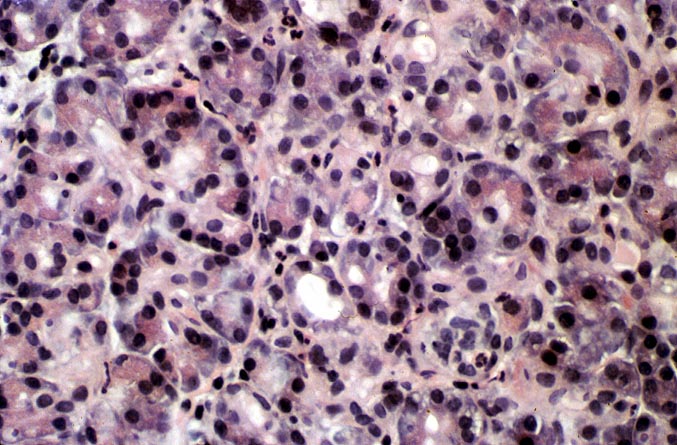



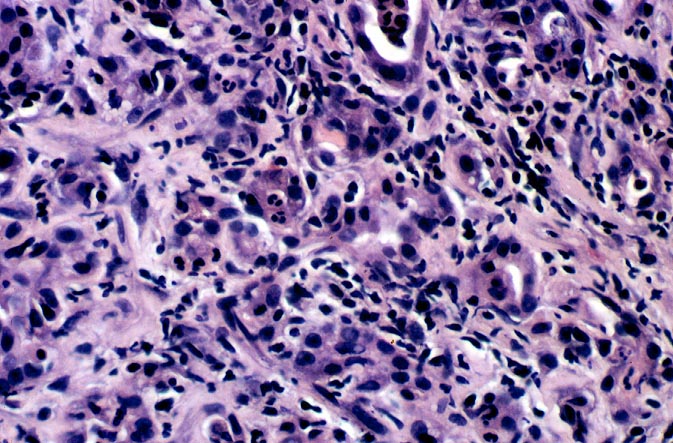
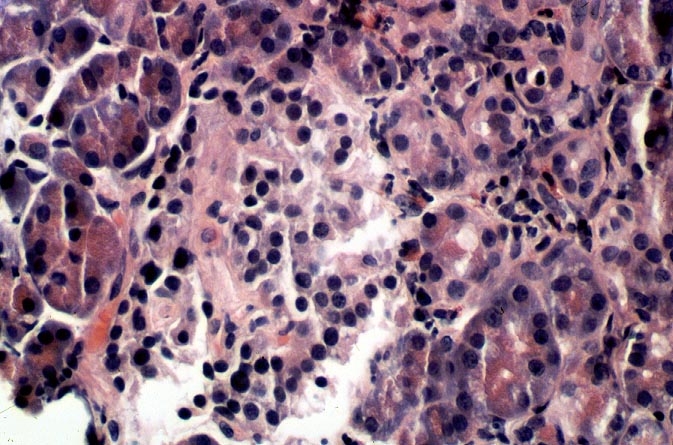
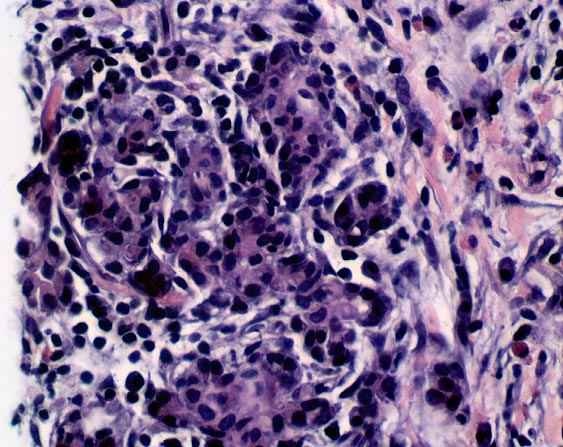
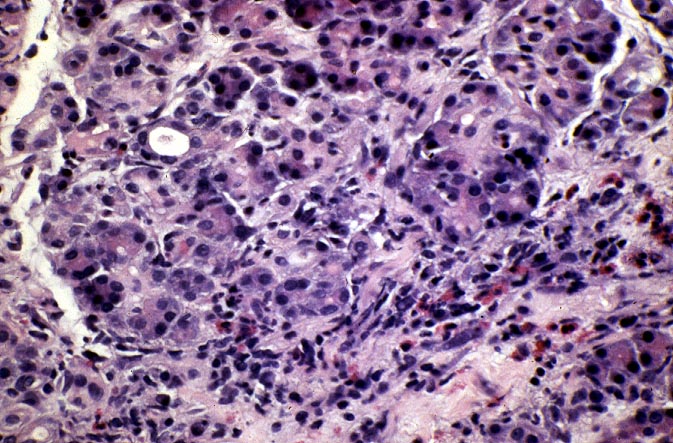

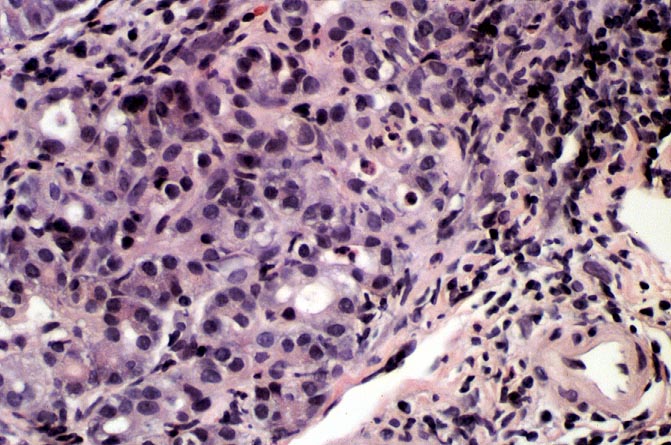
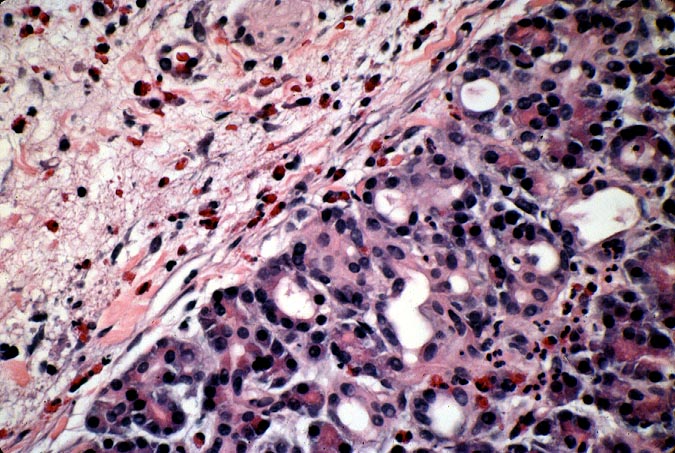
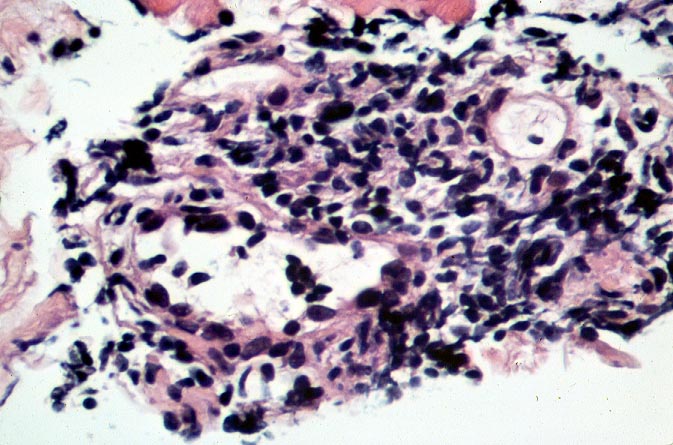
In mild rejection there are multiple foci of acinar inflammation composed predominantly of lymphocytes and eosinophils with mild evidence of acinar cell damage. The latter is manifested as drop-out of acinar cells, vacuolization and often apoptosis. If there is significant acinar damage, admixed neutrophilic infiltrates and microabscesses are not unusual. In most cases the acinar inflammation is accompanied by some degree of septal inflammation and features described in Grade II.
