SU97-260
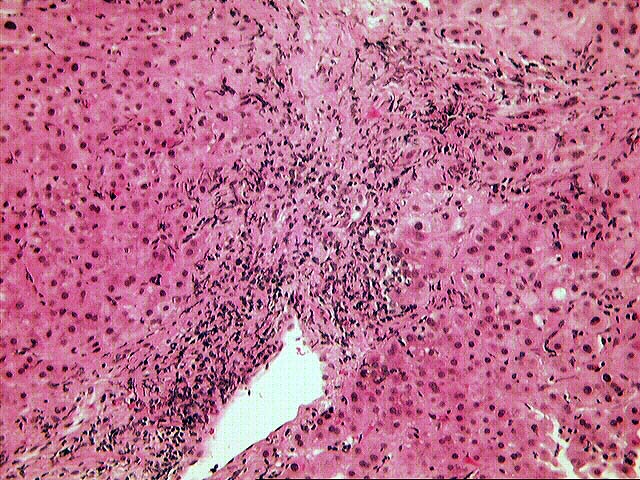
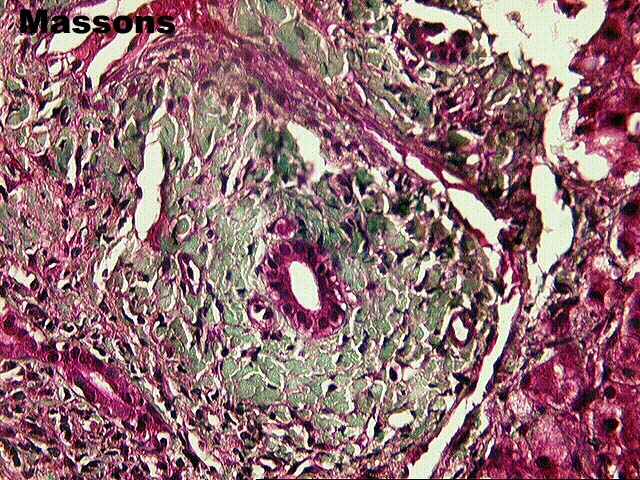
The normal lobular architecture is distorted by portal expansion,
because of fibrosis, cholangiolar proliferation and a mild to
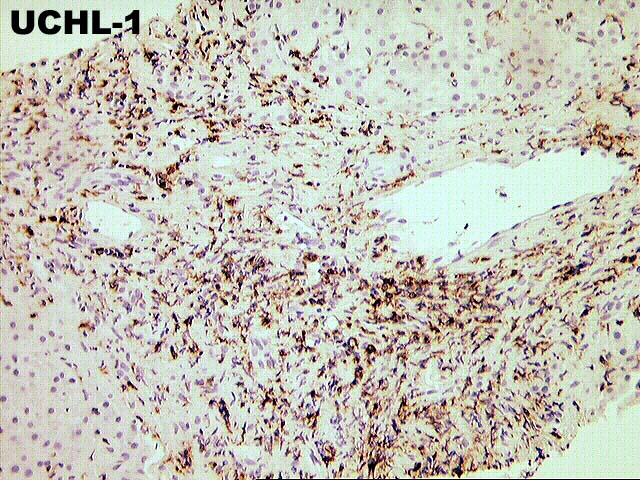
moderate mixed inflammatory cell infiltrate. Bile duct
infiltration and damage by lymphocytes is easily seen, and there
is fairly widespread atrophy and pyknosis of the biliary
epithelium. However, there is also marked interface activity,
including cholangiolar proliferation.
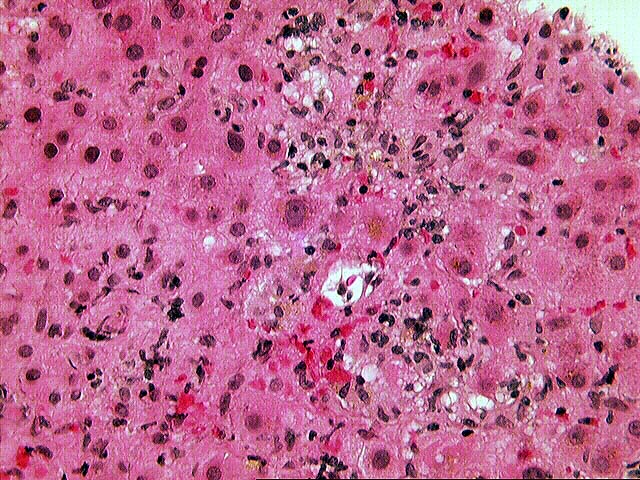
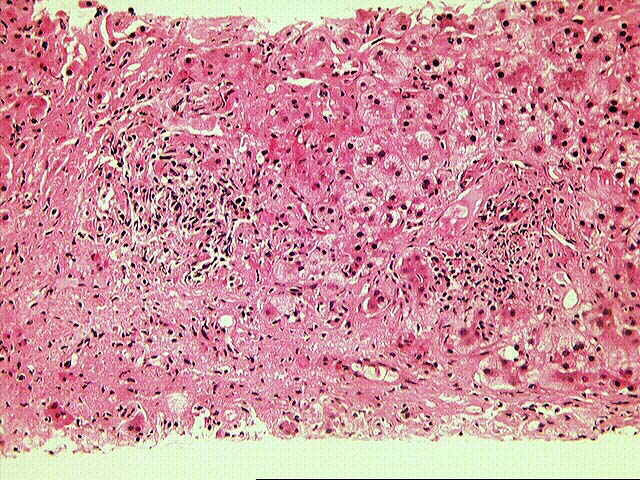
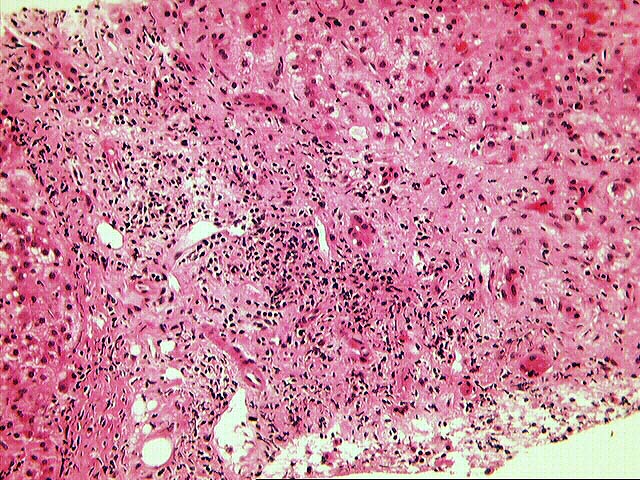
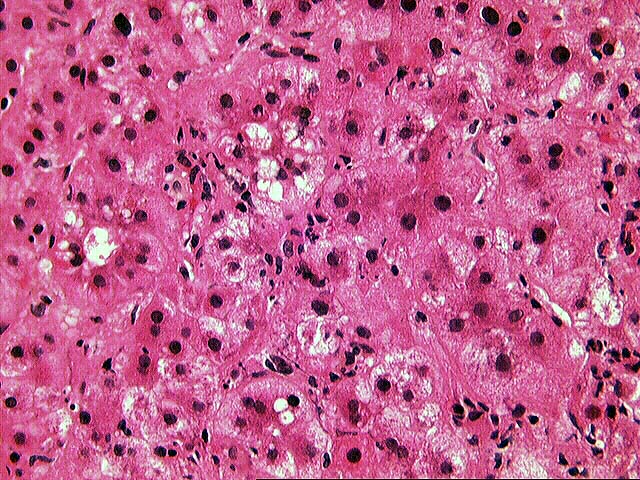
Throughout the lobules, there is moderate to severe lobular disarray, marked Kupffer cell hypertrophy, spotty acidophilic necrosis of hepatocytes and moderate to severe lymphohistiocytic lobular inflammation which is somewhat accentuated in the perivenular regions. No definite ground glass cells or other viral inclusions are detected.
SU97-498
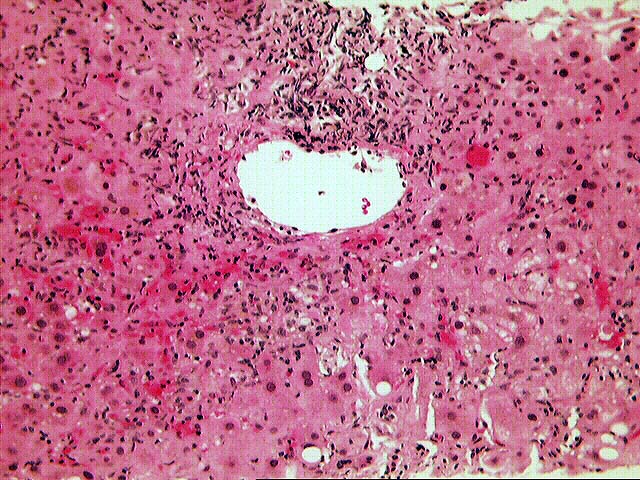
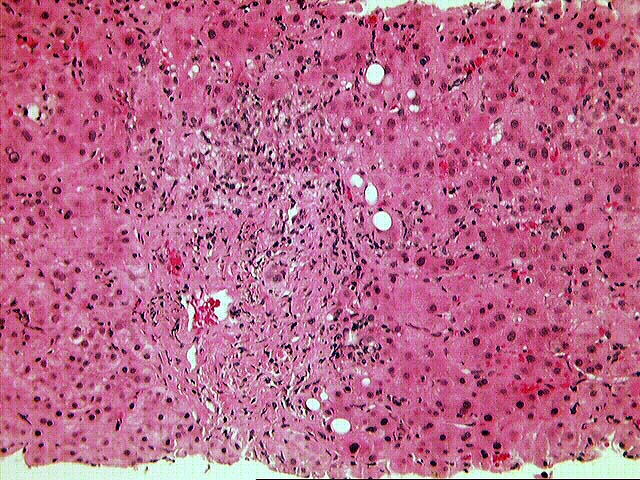
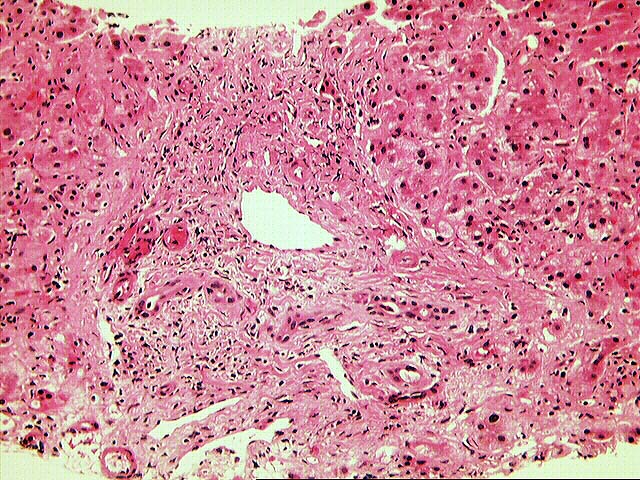
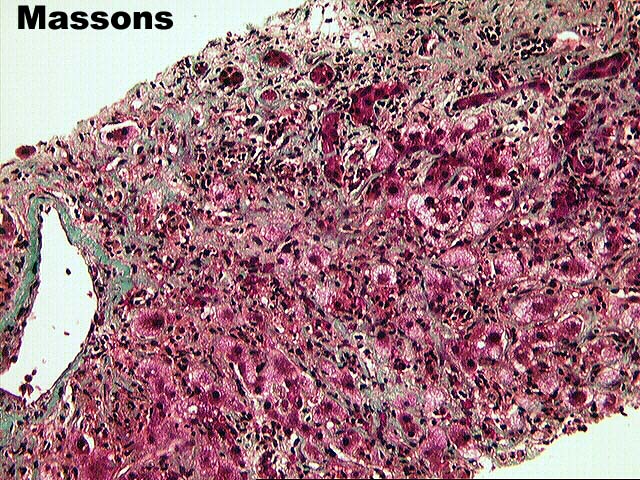
The normal lobular architecture is distorted by marked portal
expansion with focal portal-to-portal and portal-to-central
bridging fibrosis. There is also a mild, predominantly
mononuclear inflammatory cell infiltrate which is decreased
somewhat in appearance to the previously biopsy. However, there
continues to be widespread bile duct atrophy and pyknosis. This
should be reflected in fairly significant elevations of the gamma
glutamyltranspeptidase and alkaline phosphatase. In addition,
lymphocytic bile duct damage is also present.
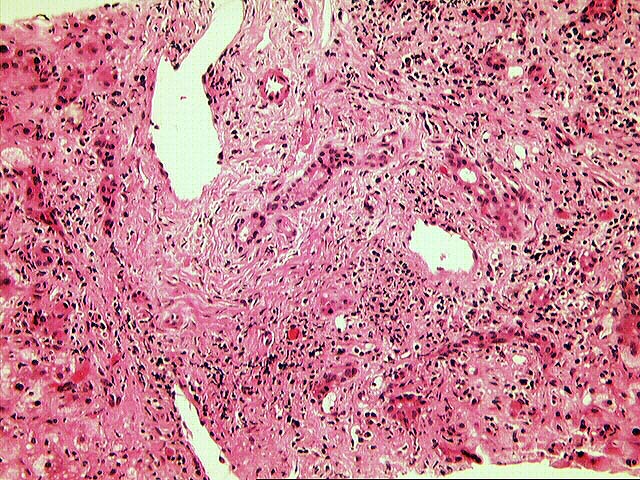
As in the previous specimen, there is mild to moderate interface activity, including cholangiolar proliferation. Throughout the lobules, there is moderate Kupffer cell hypertrophy, spotty acidophilic necrosis of hepatocytes, hepatocellular swelling and lymphohistiocytic lobular inflammation which is somewhat accentuated in the perivenular regions.
No viral inclusions or ground glass cells are seen.
Overall, the histopathological findings in both biopsies are indicative of more than one histopathologic insult. First and foremost, the most significant insult appears to be an active hepatitis. This contention is based on the mild to moderate interface activity, cholangiolar proliferation, lobular disarray, panlobular inflammation, spotty acidophilic necrosis of hepatocytes and positive PCR for HCV. However, a significant component of rejection is also present. In the first biopsy, the lymphocytic infiltration and damage of small bile ducts is far more than one would expect for hepatitis alone. In addition, there is fairly widespread bile duct atrophy and pyknosis. The slight perivenular accentuation of the lobular inflammation along with areas of selective perivenular fibrosis are also more frequently seen with rejection.
This page and its contents are Copyright © 1996, 1997 University of Pittsburgh. All rights reserved. Unauthorized redistribution prohibited.