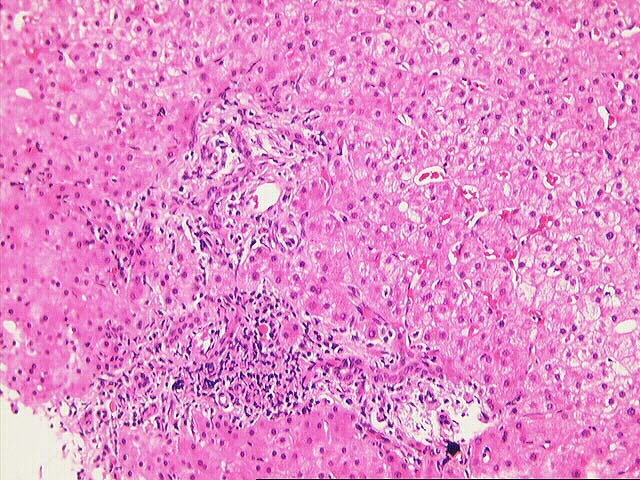
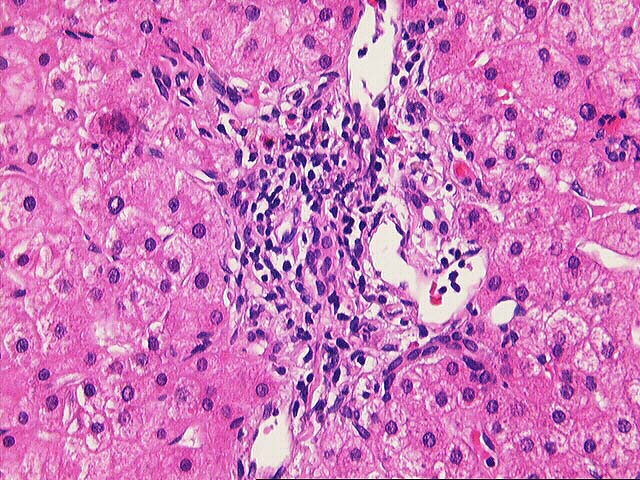
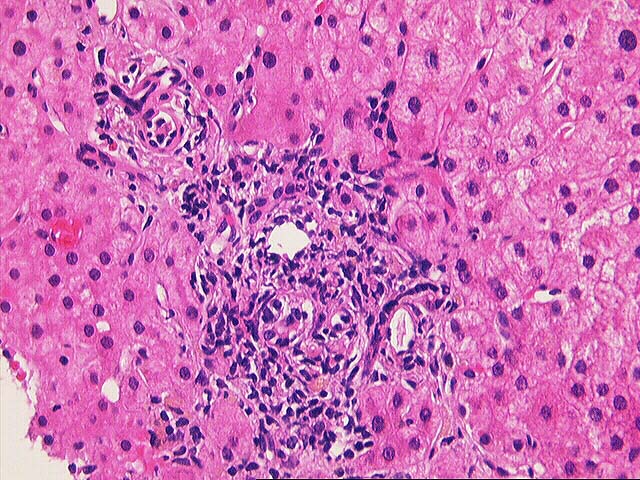
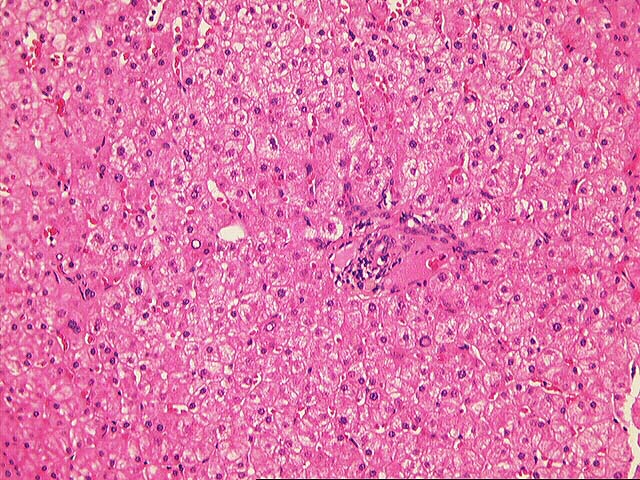
The normal lobular architecture is mildly distorted secondary to mild portal expansion because of a mild mixed portal inflammatory cell infiltrate and mild cholangiolar reactivity. Focal bile duct infiltration and damage is seen, and there is mild portal edema. However, no periductal or lamellar edema or significant cholestasis is appreciated.
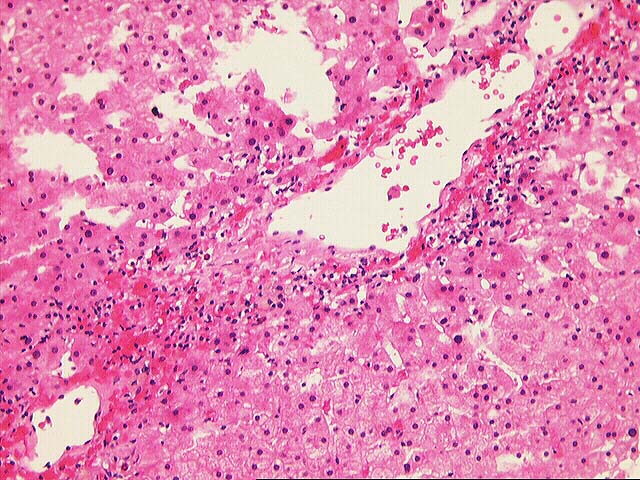
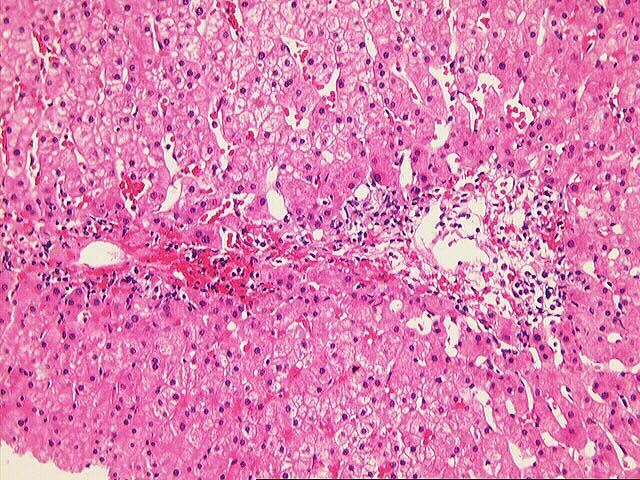
One of the most striking findings is the presence of perivenular inflammation, hepatocyte dropout and congestion. No significant lobular disarray or viral inclusions are seen.
Overall, the histopathological changes are diagnostic of mild acute cellular rejection with prominent central venulitis. While we cannot absolutely exclude a diagnosis of biliary tract obstruction or stricturing because of the mild cholangiolar reactivity and other portal changes, the centrilobular inflammation, necrosis and dropout are not seen with mechanical biliary tract problems. I look forward to any follow-up in this case.
This page and its contents are Copyright © 1996, 1997 University of Pittsburgh. All rights reserved. Unauthorized redistribution prohibited.