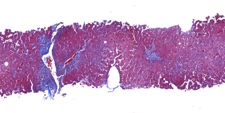
Trichrome stain shows only mild periportal fibrosis image
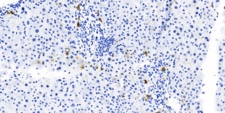
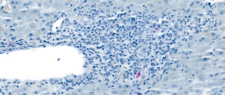
S100 immunostain shows positive uptake in an intrabiliary cell image
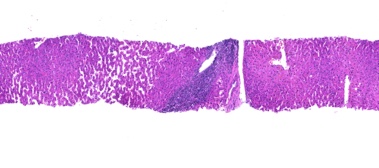
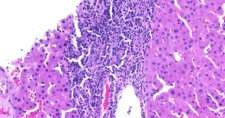
The biopsy showed a mild to moderate lymphoplasmacytic and focal eosinophilic portal inflammation with focal lymphocytic cholangitis that was thought to represent recurrent primary biliary cholangitis. Duct loss was estimated at 29%. S100 stain showed occasional intrabiliary dendritic cells and CK19 stain showed loss of Hering canals. CK7, although weak, did show some hepatocyte ductular metaplasia. Background changes of sinusoidal dilatation and vague nodularity were interpreted as a secondary nodular regenerative hyperplasia.
The Banff Working Group published a review detailing differential histologic features of various causes of late allograft dysfunction, including recurrent primary biliary cholangitis, recurrent primary sclerosing cholangitis and biliary strictures, acute and chronic rejection, chronic viral hepatitis and autoimmune hepatitis. The article is available here. A grading and staging system for primary biliary cholangitis, typically used in native liver pathology, was formulated by Nakanuma's group and is summarized here.
Please mail comments, corrections or suggestions to the
TPIS administration at the UPMC.