|
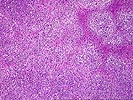
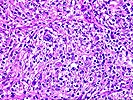
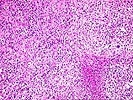
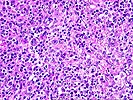
Neoplastic PTLD. Case 4. Posttransplant Hodgkin's Disease This young male received a liver transplant for relief of
sclerosing cholangitis. His underlying disease was a complication
of Crohn’s disease which had been diagnosed 8 years earlier.
His family history was positive for ulcerative colitis,
Hodgkin’s disease, leukemia, and diabetes in close family
members. Following uncomplicated liver transplant, he was
discharged under Cyclosporine/steroid immunosuppression. His only
complication was a tooth abscess two months posttransplant. Five
months after transplant he complained of throbbing flank pain,
and developed fever to 103F without chills, anorexia and fatigue.
Ultrasonography revealed paraaortic nodes in the distal aorta and
pelvis, with no adenopathy elsewhere. Urine was positive for CMV.
A lymph node biopsy was consistent with mixed cellularity
Hodgkin’s disease. A trial of reduced imunosuppression was
initiated. The patient returned to his home state and was
apparently well for another 4 years, at which time recurrence of
a histologically similar tumor occurred. Few details of this
hospitalization are available at present, but he apparently
received chemotherapy for Hodgkin’s disease. The patient
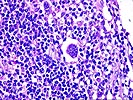
expired 3.5 years following the original tumor diagnosis. The
slide series is taken from the original node biopsy and shows
effacement by a mixed cell infiltrate consistent with
Hodgkin’s disease. The infiltrate extended beyond the
capsule, and in some areas residual node elements were
identifiable. Reed-Sternberg and Hodgkin cells were easily
identified. Focal necrosis was observed (the patient had not
received chemotherapy prior to this biopsy). Eosinophils were
focally prominent and an example is given here. The large
atypical cells were positive for EBV by the EBER stain. These
cells were also among the replicating cells according to
immunostain for cell cycle-associated antigens. Molecular clonal
studies were not available. Note: Click on the thumbnails to view the microscopy of this case- the "up" arrow will take you to the top of the page to see them again. Click on the back arrow to return to the previous case or the forward arrow to go to the next case. Please mail comments, corrections or suggestions to the TPIS administration at the UPMC. University of Pittsburgh. All rights reserved. Unauthorized redistribution prohibited.
If you have more questions, you can always email TPIS Administration. |
||||