


|
Islet Cell Drug Toxicity 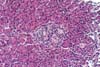





The use of more potent
immunosuppressive drugs such as cyclosporine and tacrolimus has markedly
improved the outcome in pancreas transplantation. In addition to nephrotoxicity, hirsutism/alopecia, neurological and gastrointestinal side
effects, both these drugs can cause abnormalities in glucose metabolism.
Hyperglycemia is more commonly seen in patients receiving tacrolimus. In the pre-cyclosporine era secondary to the use of large doses of
corticosteroids, post-transplant diabetes mellitus occurred in almost half of
renal transplant patients. Older age,
higher body weight, family history of abnormal glucose metabolism and
African-American or Hispanic descent are associated with higher incidence of
post-transplant diabetes mellitus. The latter is believed to result from
insulin resistance with a relative deficiency of insulin. Insulin resistance
results from decreased insulin receptor number and affinity, inpaired glucose
uptake and probably inhibition on insulin secretion by beta cells. In animal studies cyclosporine administration has been associated with
reduction in insulin secretion, diminished beta cell density, decreased insulin
synthesis and defective insulin secretion. Similar morphological
findings have been seen also with tacrolimus.
The incidence of hyperglycemia in patients receiving cyclosporine and
tacrolimus is considered to be 11-19% and 15-29% respectively. Most patients
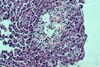
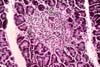
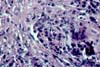
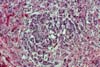
also receive steroids and this is a confounding factor. The morphological findings in biopsies from patients with clinical
evidence of drug toxicity consist of cytoplasmic swelling and vacuolization of
islet cells. The islets appear clear and stand-out from the more eosinophilic
acinar parenchyma. In more severe cases islet cell drop-out with formation of
spaces (lacunae) can be seen if there is confluent islet cell drop-out. Rarely, apoptotic cell fragments can be
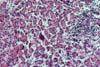
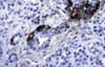
identified. Immunoperoxidase
stains for insulin and glucagon shows diminished staining for insulin in beta
cells in comparison to controls. This is the light microscopic counterpart of
the marked loss of dense core granules seen in beta cells by electron
microscopy. The latter study shows preservation of the peripheral non-beta
cells in the islets. The histological changes and the clinical findings are reversible with
reduction or discontinuation of the drug. In our experience, hyperglycemia and
the histological evidence of drug toxicity was worsened with the concurrent use
of pulse steroids to treat acute rejection.
Trials are being conducted to achieve steroid free immunosuppression in
pancreas transplantation. The typical clinical scenario in drug toxicity consists of a patient
presenting with hyperglycemia in association with higher than desired levels of
tacrolimus or CSA. The biopsy usually
shows no evidence of significant acute or chronic rejection. Glycemia should normalize after reduction of
drug level. References Drachenberg CB,
Klassen DK, Weir MR, Wiland A, Fink JC, Bartlett ST, Cangro CB, Blahut S,
Papadimitriou JC: Islet cell damage assosociated with tacrolimus and
cyclosporine: Morphological features in pancreas allograft biopsies and
clinical correlation. Transplantation 1999;68:396. Mayer AD, Dmitrewski
J, Squifflet JP et al.: Multicenter randomized trial comparing FK506 and
cyclosporin in the prevention of renal allograft rejection: a report of the
European FK506 Multicenter Renal Study Group. Transplantation 1997;64:436. HiranoY, Fujihara S,
Ohara K, Katsuki S, Noguchi H: Morphological and functional changes in islets
of Langerhans in FK506-treated rats. Transplantation 1992;53:889. Tze WJ, Tai J,
Murase N, Tzakis A, Starzl TE: Effect of FK506 on glucose metabolism and insulin
in normal rats. Transplant Proc 1991;23:3158. Krentz AJ, Dousset
B, Mayer D, et al.: Metabolic effect of cyclosporine A and FK506 in liver
transplant recipients. Diabetes 1993;42:1753. Stratta RJ: Review
of immunosuppressive usage in pancreas transplantation. Clin Transplant
1999;13:1. Jordan ML,
Chakrabarti P, Luke P, et al.: Results of pancreas transplantation after
steroid withdrawal under tacrolimus immunosuppression. Transplantation
2000;69:265.
If you have more questions, you can always email TPIS Administration. |
|