Antibodies reactive with donor antigens can have many different
effects on an allograft: they can destroy it, enhance its survival,
or have no effect on the function of an allograft(1). The final
determinants include the class, titer and specificity of the anti-donor
antibodies, the timing of the response; the density and distribution
of target antigens in the organ(1, 2) and possibly, on the source
of complement. Only those antibody systems capable of causing
damage will be covered below.
Humoral rejection of the liver has recently been defined by the
WORLD CONGRESSES OF GASTROENTEROLOGY consensus document(3) as
"a relatively uncommon form of allograft injury and subsequent
dysfunction, primarily mediated by antibody and complement, occurring
immediately (hyperacute) or during the first week (acute) after
transplantation. The antibodies are either preformed antibodies
or represent anti-donor antibodies that developed after transplantation."
This panel(3) considered acute humoral rejection, antibody mediated
rejection and hyperacute rejection as acceptable synonyms.
Historically, it has been difficult to attribute liver allograft
damage to preformed antibodies(4-9). This was largely because
of a well-documented resistance of the liver to humoral rejection
in comparison to kidney or heart allografts(2, 4-13). In addition,
many "non-immunologic" complications, such as preservation
injury and sepsis, can also produce a clinicopathologic syndrome
quite similar to humoral rejection (14-16). Comparatively poor
survival rates early after liver transplantation during the advent
of clinical liver transplantation also made it
difficult to correctly identify those who died or required retransplantation
because of antibody mediated injury(16). With improvements in immunosuppression,
patient selection, operative techniques and patient management, it is now clear
however,
that antibodies directed against the major ABO blood group antigens(14,
17-19) and MHC antigens(1, 20-26) can cause allograft failure,
albeit rarely in a "hyperacute" fashion.
The first system to be described that predictably resulted in
humoral hepatic allograft rejection was the major ABO blood group
isoagglutinins(14, 17-19). Once this barrier was recognized, crossing
the ABO blood groups in liver transplantation was generally avoided
and humoral rejection because of a major blood group incompatibility
became rare. However, in candidates with fulminant hepatic failure
where the need is urgent or in children, where the donor pool
is limited, preconditioning of an ABO incompatible recipient has
been used. Various combinations of splenectomy, cytoreductive
therapy, prophylactic anti-lymphocyte globulins(27), OKT3(28,
29) and pre- or post-transplant plasmapheresis(27) have yielded
acceptable graft and patient survival results(30). Therefore,
while ABO incompatibility poses a definite risk of humoral and
acute cellular rejection, it is not considered to be an absolute
contraindication to transplantation by some groups(29).
The potential of lymphocytotoxic antibodies, which are primarily
of the IgG class, to cause liver allograft damage and failure
has been more recently recognized by several centers(1, 23-26,
31-33), but not by others(31, 34, 35). Thus, there is no general
agreement therefore, on the importance of a prospective crossmatch
in liver transplant recipients(35). However, even though lymphocytotoxic
antibodies do not usually precipitate hyperacute rejection and
are clearly less destructive than the isoagglutinins in clinical
practice, data from experimental animals clearly show that antibody-mediated
rejection alone, or in combination with acute cellular rejection
significantly contribute to liver allograft damage (1). Thus,
knowing that the recipient harbors potentially destructive preformed
antibodies is likely to be helpful for patient management in the
early post-transplant period.
Pathophysiology
Antibodies directed at antigens expressed on the vascular endothelium
are potentially the most destructive, since vascular injury interferes
with the blood supply(1). Antibodies included in this group are
those reactive with the major ABO blood group and class I MHC
antigens, detectable in conventional blood typing and lymphocytotoxic
crossmatch tests, respectfully. In xenotransplantation, polysaccharide
antigens on the surface of endothelial cells are a major barrier
to successful engraftment(36, 37).
Studies in experimental animals have provided important information
about the mechanisms of enhanced allograft damage in presensitized
recipients. Qian et al(38) have shown in experimental animals
that MHC class I rather than class II molecules play an important
role in allosensitization. The presensitization is likely related
to an augmentation of the TH1-type cytokines and immune responsiveness(39).
These observations are consistent with the clinical findings that
alloimmune antibodies of the IgG class are the most destructive(2,
40).
The critical event in the effector phase of humoral rejection
appears to be antibody binding to the endothelium and subsequent
complement fixation and activation. This results in direct endothelial
damage, the formation of platelet-fibrin thrombi, initiation of
the clotting cascade, subsequent microvascular thrombosis and
arterial vasospasm, all of which act in concert to ruin the microvasculature,
impair blood flow and eventually cause hemorrhagic necrosis.
The well-known resistance of the liver to humoral rejection has
provided important insights about the pathophysiology of humoral
rejection. Secretion of soluble MHC Class I antigens by the liver,
Kupffer cell phagocytosis of cytotoxic antibodies, complement,
immune complexes and activated platelet aggregates; the dual hepatic
blood supply through the hepatic artery and portal veins and the
unique hepatic sinusoidal microvasculature, which is devoid of
a conventional basement membrane(1, 10, 11, 13, 41-45) have all
been cited as explanations for the liver's ability to withstand
the impact of pre-formed anti-donor antibodies much better than
other organs. Recently, observations in liver xenotransplantation
have shown that compatibility of complement components is yet
another explanation for the hepatic resistance to humoral rejection(36,
46). It is known that complement mediated lysis of a target is
less effective if the target cell and complement are derived
from the same source (donor versus recipient species), than if
they are from different sources. Thus, by providing syngeneic
complement, a liver may protect it's own endothelial cells from
the complement mediated lysis triggered by the preformed antibodies(36,
46). Whether this form of protection is operable in allografts
has yet to be determined with certainty.
Even though all of these mechanisms can protect a liver allograft
from antibody mediated damage, Knechtle et al(47), Gubernatis
et al(48) and others(2) have clearly shown in animals that they
could be overridden by intense presensitization. Nakamura et al(44) have
recently outlined the events of humoral rejection in a clinically
relevant small animal model. Some of the earliest morphological
signs of humoral rejection are the presence of platelet-fibrin
thrombi in the sinusoids
, portal and
central veins. These appear within
one to three minutes after transplantation and are even better illustrated in
plastic-embedded sections and through
ultrastructural analysis. Within
one to three hours, endothelial hypertrophy and vacuolization,
spotty acidophilic necrosis of hepatocytes,
and neutrophilic portal venulitis appear. In
6-24 hours, small areas of hepatocyte necrosis
are evident and can become confluent. If the
preformed antibodies are high titer, IgG and show endothelial specificity(2),
then rapid graft failure from widespread hemorrhagic necrosis can occur.
However, if the protective mechanisms, described above, can override the
damage, gradual resolution of the platelet-fibrin
thrombi occurs during the next three to
twenty four hours after transplantation.
If the allograft does not precipitously fail,
acute (cellular) rejection frequently
develops earlier than it normally would, in non-sensitized recipients.
Clinical Presentation
The International Panel referred to earlier describes humoral
rejection as severe allograft dysfunction without an obvious cause
occurring in a presensitized patient immediately after or during
the first week after transplantation(3). The allograft may become
swollen, cyanotic, and mottled; bile production may slow or stop.
Establishing the diagnosis requires that conditions such as
"preservation"
injury, hepatic artery or portal vein thrombosis, or venous outflow
obstruction can be excluded with reasonable certainty. Depending
on the severity of injury, the above findings may be accompanied
by a consumptive coagulopathy and operative site bleeding, with
a need for blood components(3).
ABO Incompatible: The first signs of serious liver injury
often develop in the operating room after vascular re-anastomosis
and before abdominal closure(14, 18, 19, 49, 50). The liver usually
reperfuses uniformly and produces bile, but within minutes or
hours becomes hard and swollen before bile flow slows or stops
altogether. An inordinate need for platelets and difficulty in
achieving hemostasis signal the initiation of an intrahepatic
consumptive coagulopathy (40). However, the intra-operative events
are rarely serious enough to abort the procedure or undertake
immediate retransplantation. An unexplained rise in liver injury
tests during the first several post transplant days, refractory
thrombocytopenia, hypocomplementemia and symptoms signal the possibility
that humoral rejection is occurring(14, 19, 40, 49, 50). At this
point,
hepatic angiography is often obtained to investigate the
cause of the unexplained allograft dysfunction. In the typical
case, it shows segmental narrowing, or a "sausage-link"
appearance(14, 19, 21, 49, 50) and/or diffuse luminal narrowing
with poor peripheral filling. These are signs indicative of
immunologically-mediated
arterial vasospasm.
Unfortunately, in conventionally treated recipients of ABO incompatible
organs the marked rise in transaminases is followed in 60% - 70%
of cases by synthetic function failure, subsequent wound site
bleeding and other systemic signs of hepatic failure, that necessitate
retransplantation(14, 19, 21, 49, 50). Those that survive the
early insult are more prone to the development of biliary tract
strictures late after transplantation(14, 51).
ABO Compatible: Lymphocytotoxic antibodies in general,
cause less serious injury than the isoagglutinins(1, 20-26, 40).
In addition, the ability of various lymphocytotoxic antibodies
to effect graft damage greatly varies, which appears to be related
to the antibody titer, specificity and class(2, 40, 44). The IgG
class reportedly cause the most damage(1, 20-26, 40). In addition,
one cannot exclude the possibility that the use of blood products
containing anti-donor antibodies and active complement can contribute
to the injury.
In general, the higher the titer of IgG anti-MHC antibodies detected
on the routine crossmatch before transplantation(23, 25, 26) the
more likely the patient will encounter significant difficulties
during and after the operation(2, 40, 44). However, the relative
risk to the recipient and the potential number of patients involved
should be kept in perspective. Crossmatch positivity for IgG lymphocytotoxic
antibodies is typically encountered in 8 -12 % of all liver allograft
recipients, and of those, only 30% have more dangerously high
titers(40). Thus, the patient population at greatest risk is relatively
small (23, 26, 40) and in a liver transplant program where there
are fewer than 100 cases per year, humoral rejection may be overlooked
as a cause of dysfunction or failure.
The most frequent clinical presentation is a persistent rise in
serum bilirubin that occurs during the first week after transplantation,
accompanied by refractory thrombocytopenia(52), low complement
activity, and a biopsy showing changes of "preservation injury"(40).
This is usually followed by the onset of
acute (cellular) rejection and the need for increased
immunosuppression(1, 2, 44).
Ischemic biliary necrosis later manifest as
biliary sludge,
obstructive cholangiopathy and small bile duct loss are other serious late
manifestations(1, 2, 44, 51, 53). In rare cases, precipitous hemorrhagic
necrosis similar to that seen with isoagglutinins can occur(32).
Gross and Histopathology
The diagnosis of humoral liver allograft rejection is difficult to
establish with certainty, and implies that other causes
of early liver allograft failure such as preservation injury,
vascular compromise, sepsis and trauma have been reasonably
excluded. This usually requires a "backtable" liver biopsy that
shows no significant
steatosis,
portal inflammation,
hepatocyte necrosis or
immunoglobulin deposits.
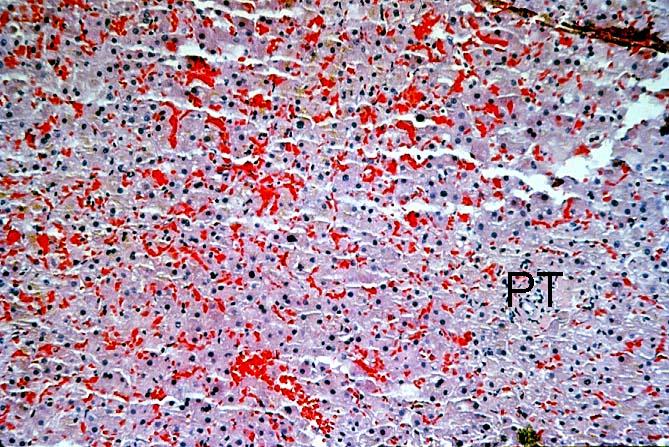
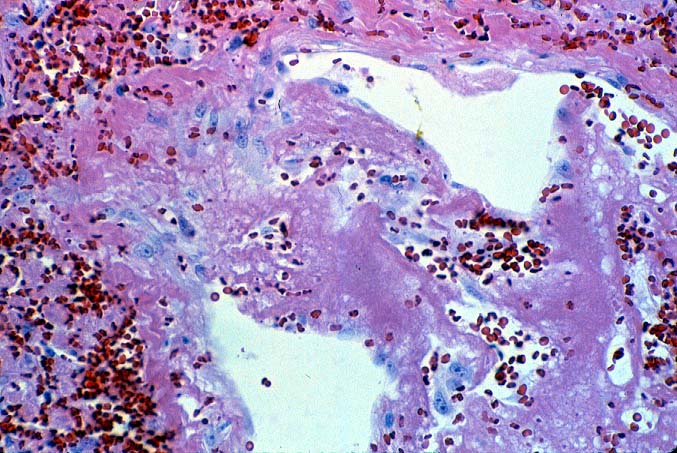
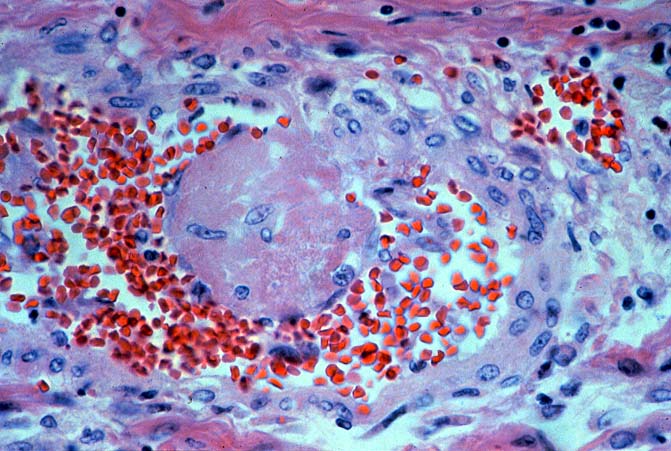
ABO Incompatible Organs: The histopathologic findings depend
on the timing of the biopsy and the severity of the injury. Samples
taken immediately after reperfusion from patients with marked
injury may show an impressive
sludging of red blood cells and
a clustering of neutrophils in the sinusoids. Focal platelet-fibrin
thrombi in portal and central veins can also be seen. Hemorrhage
into the space of Disse',
small areas of ischemic hepatocellular
necrosis usually follow within the next
hours to days(14, 19, 49, 50).
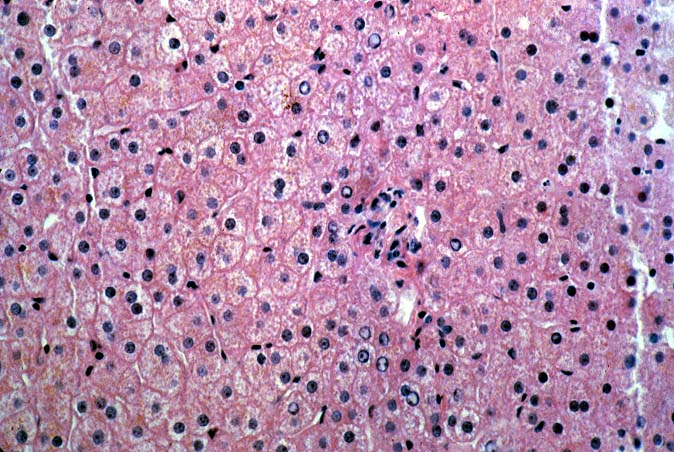
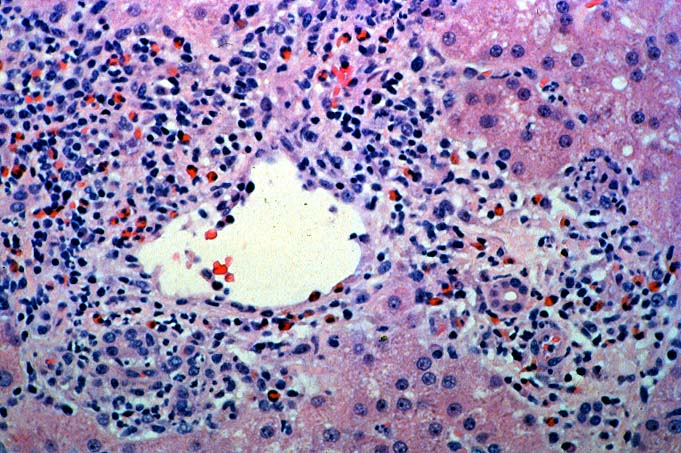
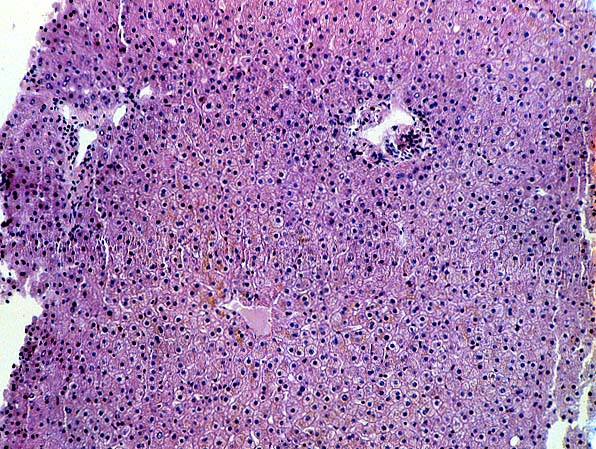
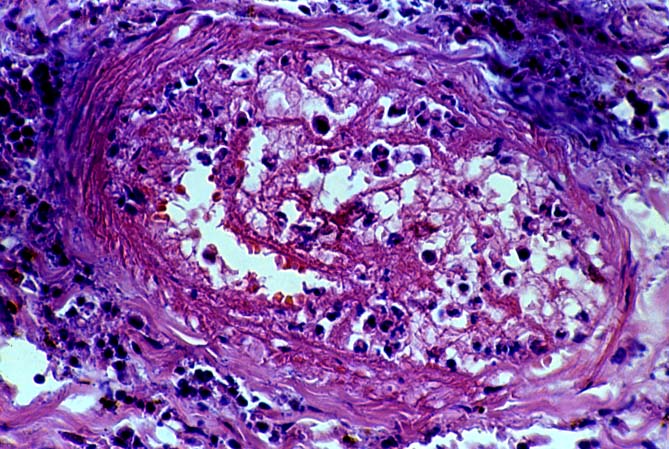
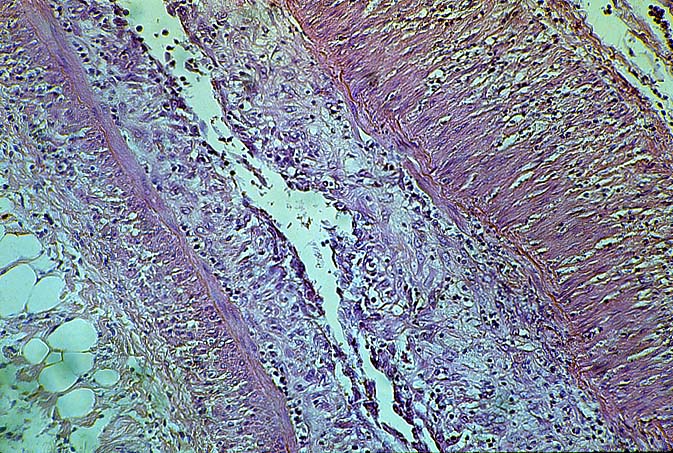
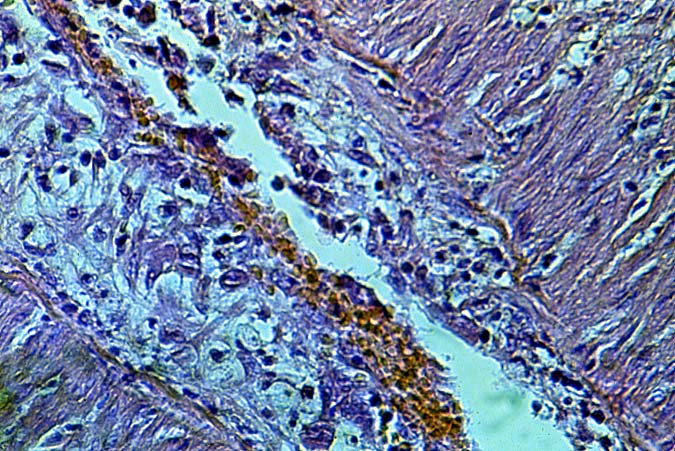
Biopsies taken within the first several days in those with severe
injury will show confluent coagulative hepatocyte necrosis without
any particular lobular distribution. Nearby portal veins contain
circumferential fibrin deposition
and markedly hypertrophic endothelial
cells. Arteries are usually less severely affected, although neutrophilic
and/or necrotizing arteritis
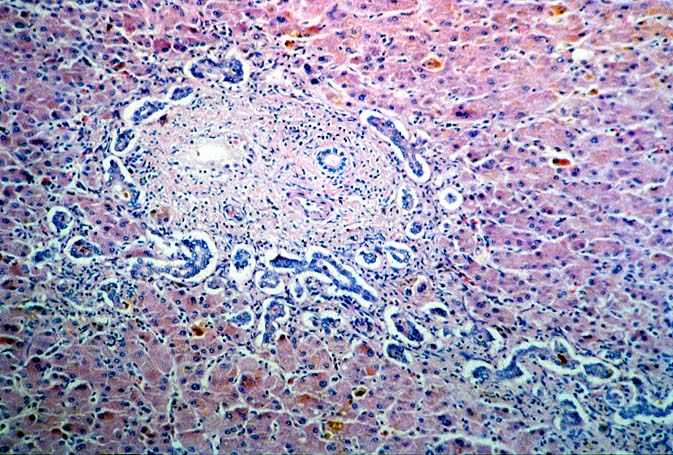
can be seen on occasion. A mild neutrophilic
portal exudate usually appears at 2 to 3 days, as does focal cholangiolar
proliferation. The latter finding is interpreted as a hepatic
response to injury in the periportal region. Thereafter,
progressive hemorrhagic infarction of the organ occurs in patients destined
for allograft failure(14, 19, 49, 50).
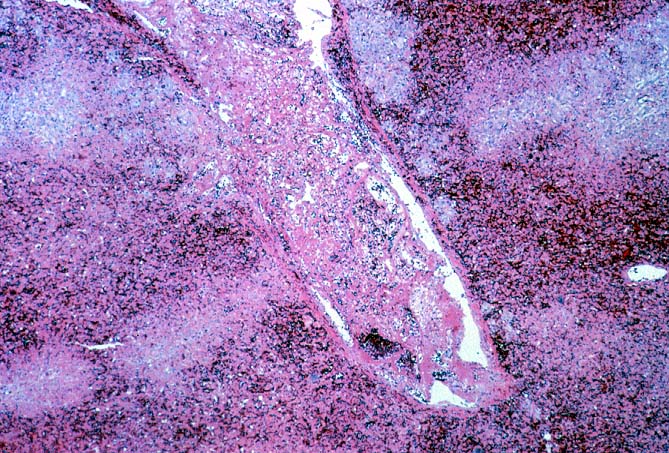
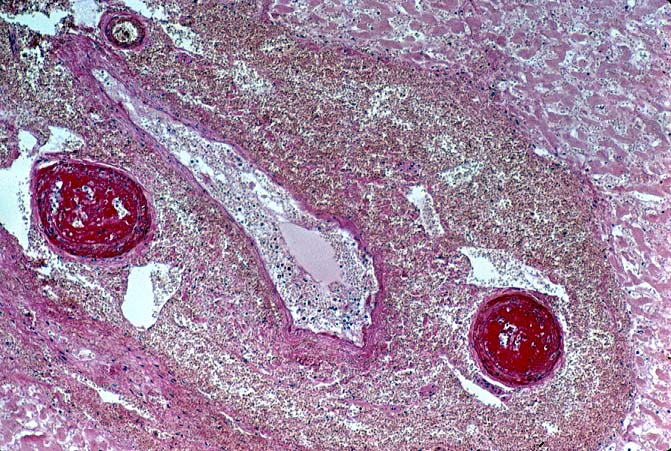
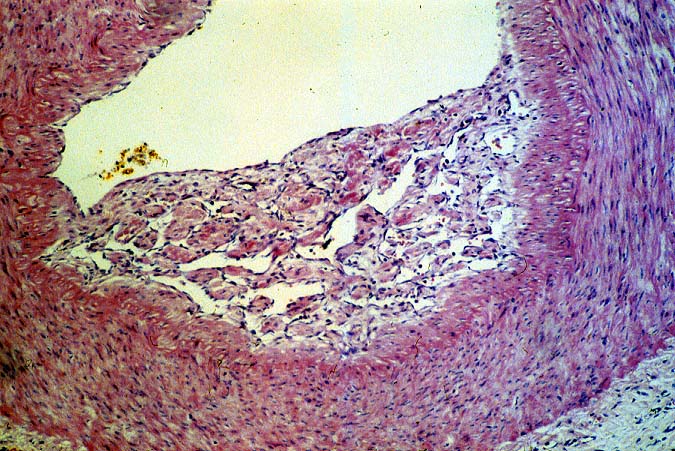
Failed ABO incompatible allografts
examined at the time of retransplantation
often reveal enlarged, cyanotic organs, mottled with areas of
necrosis(14, 49), with or without rupture of the capsule. Hepatic
artery and portal vein thrombosis is variably present. Microscopically,
large
geographic areas of hemorrhagic necrosis are the most frequent
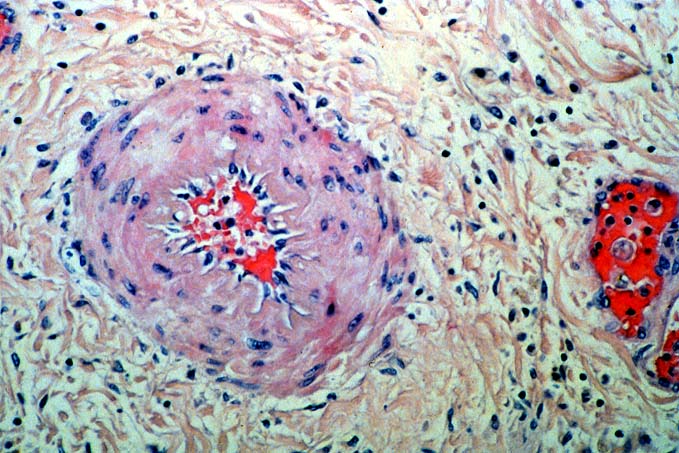
findings. On closer examination, focal fibrinoid necrosis of arteries
may be seen but is present in only a minority of cases. More common
vascular findings include
arterial and venous endothelial cell
hypertrophy, neutrophil sludging, focal fibrin deposition around
a partial circumference of the vessel, with a
mass of fibrin extending into the lumen (14, 49).
The presence of arterial medial thickening
and myocyte vacuolization are common and probably represent morphologic
manifestations of arterial vasospasm.
In addition, a rapidly developing fibro-intimal
hyperplasia can occur.
Occasionally, if the allograft survives the first week after
transplantation the injury will subside. However, there is an
increased risk of long term biliary tract strictures, presumably
related to residual arterial pathology, such as
re-canalized thrombi.
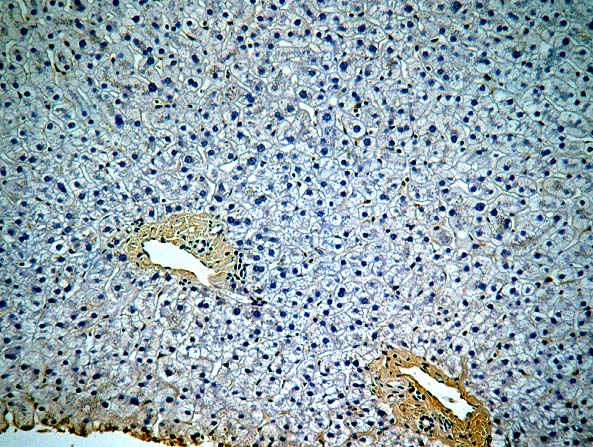
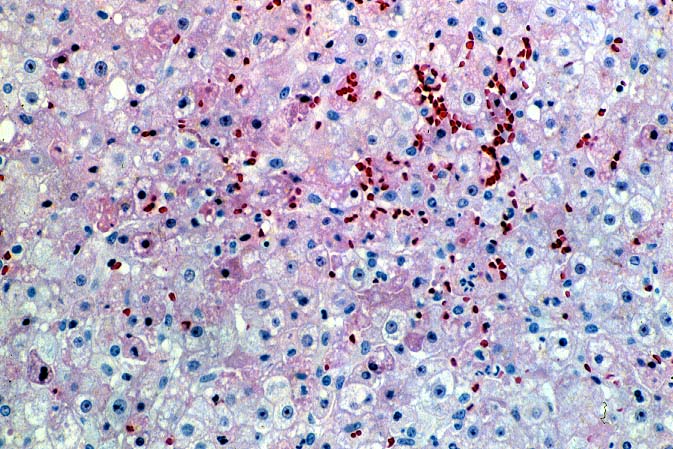
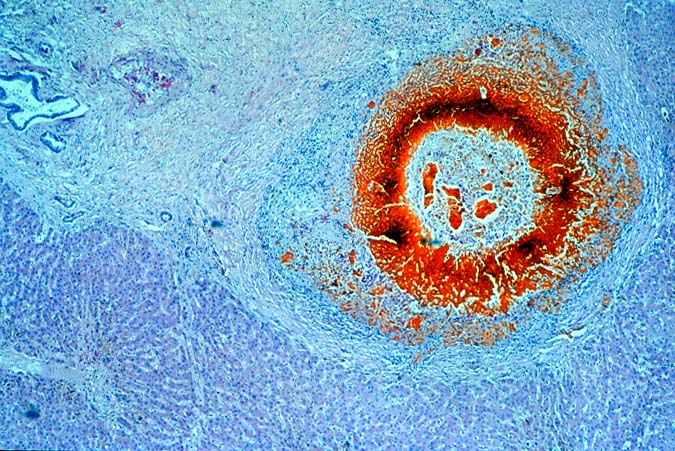
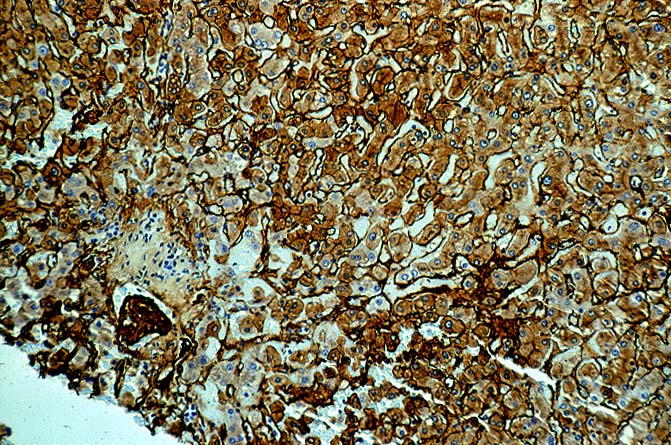
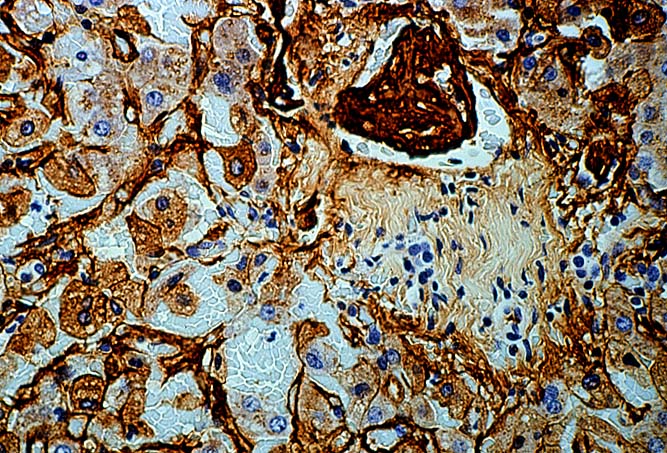
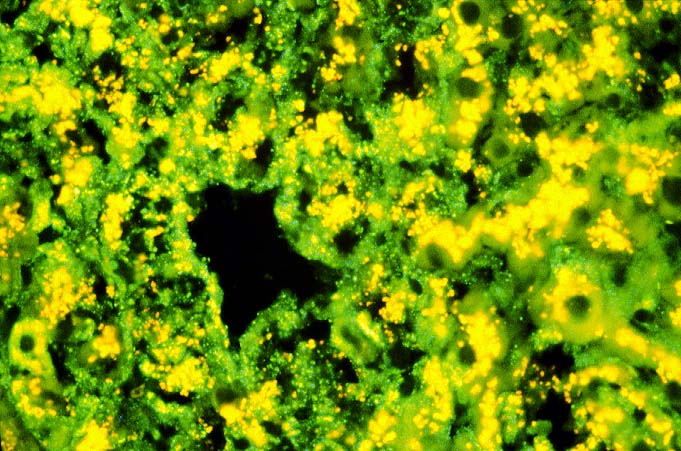
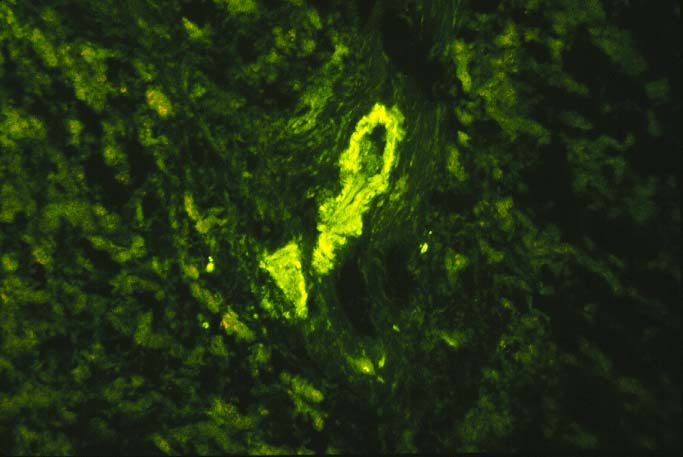
Immunofluorescent
and immunoperoxidase stains in
ABO incompatible organs will often reveal IgM, focal IgG, C3, C4 and Clq
in an occasional artery,
in the hilar microvasculature and in the
sinusoids.
However, arterial deposits of IgG, IgM and Clq may be seen in
a similar distribution in allografts with non-immunologically
mediated injury. Background fluorescence
in the portal connective tissue and sinusoids can present a problem
during interpretation of the findings. Elution studies can be performed to
confirm the identity of the deposited antibodies(14, 49). The final diagnosis
should be based on a complete clinicopathologic analysis during
which other non-immunologic causes of graft failure are reasonably
excluded.
ABO Compatible Organs: In general, the hepatic damage is
more variable and generally less severe in patients with a positive
crossmatch than in those with incompatible isoagglutinins. In
addition, the injury pattern is more often difficult to separate
from other insults that mimic humoral rejection. In the typical
clinical case, reperfusion biopsies from patients with a positive
lymphocytotoxic crossmatch more often contain platelet aggregates
in the portal and or central veins than crossmatch negative controls(1,
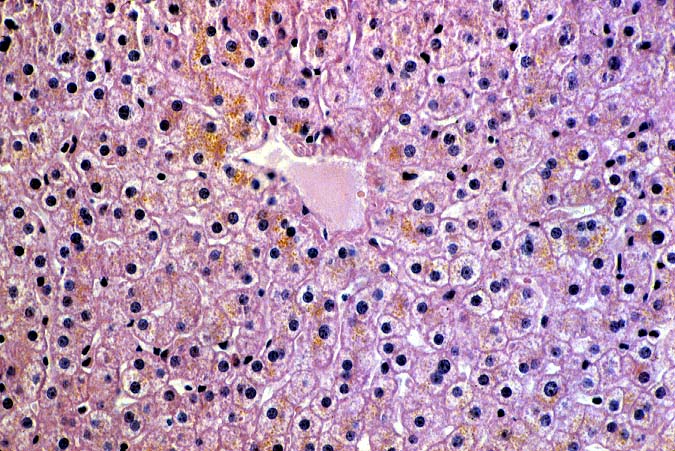
44). Spotty acidophilic necrosis of hepatocytes, centrilobular
hepatocellular swelling, accompanied by cholangiolar proliferation
and hepatocanalicular cholestasis often appear during the first
week after transplantation. Neutrophilic or necrotizing arteritis
is rare(1, 44) in needle biopsy specimens, but lymphocytic subendothelial
infiltration is not uncommon in large hepatic artery branches.
Overall, the histopathologic changes closely resemble those of
"preservation" injury, except for subtle arterial changes,
which also may not be present in needle biopsy samples. These
are best observed in arteries from the perihilar region of allograft
hepatectomy specimens and include endothelial hypertrophy, lymphocytic
arteritis, medial thickening, partially organized thrombi, necrosis
of individual myocytes, and medial myocyte vacuolization(1, 44).
Other hilar changes in humoral rejection include congestion of
the peribiliary vascular plexus and
biliary necrosis of large septal bile ducts(1, 44).
If allograft failure does not occur in a positive crossmatch patient,
acute rejection
, manifest as cellular infiltration of the liver,
usually becomes evident within 5 - 7 days of transplantation(1,
44). This makes the cause of injury and dysfunction more obvious.
If the allograft survives the early post-operative injury, long
term sequela of an early humoral insult either from isoagglutinins
or lymphocytotoxic antibodies can include:
biliary sludge and stricturing with obstructive cholangiopathy, and
obliterative arteriopathy and
loss of small bile ducts, or
chronic rejection(14, 19, 27, 51).
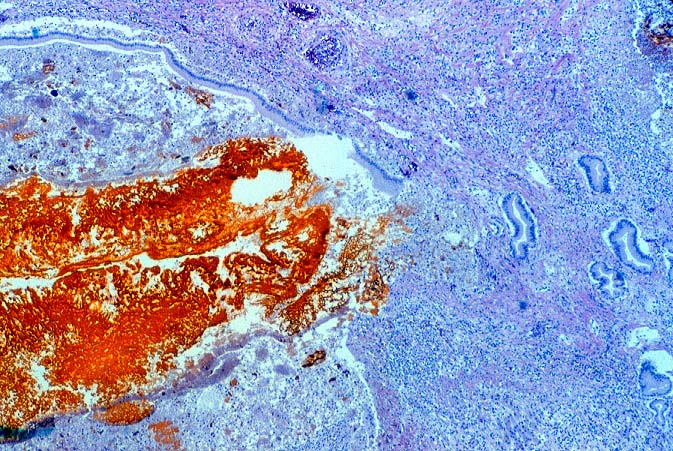
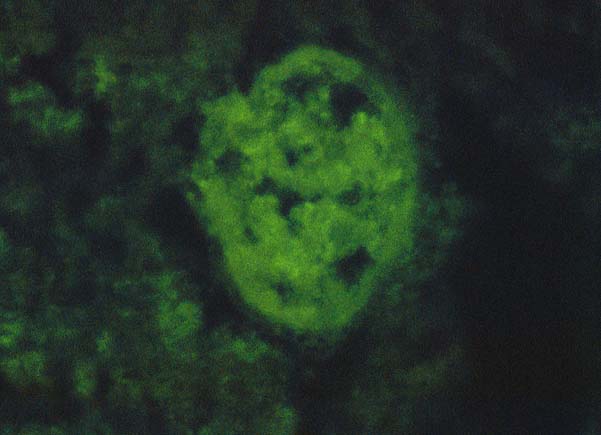
In our experience, the immunofluorescence findings in ABO compatible
allografts can be supportive of humoral rejection, but alone,
they rarely are diagnostic unless the immune deposits are intense.
Deposits of IgG, C3 and C4 in the arteries and in the portal and
hilar microvasculature, without heavy a-2-macroglobulin
or other macromolecules suggest specific deposition. Therefore,
such deposits are more indicative of humoral rejection than are
"non-specific" localization of IgM, Clq and other macromolecules,
which frequently become lodged in necrotic arterial walls, regardless
of the cause of damage.
The International Panel suggests that the minimal diagnostic
criteria are: rapid onset liver dysfunction with histologic
features of ischemic necrosis and predominantly neutrophilic infiltrates,
in the absence of other clearly defined causes of ischemia or
infarction. The diagnosis is strengthened if neutrophilic or necrotizing
arteritis is present, if immunoglobulin deposits can be demonstrated
in the liver, and if preformed anti-donor antibodies are found.
Technical and preservation-related causes of ischemia infarction
should be reasonably excluded(3).
Differential Diagnosis
Severe humoral rejection can easily be confused with other insults
that cause hemorrhagic hepatic necrosis, such as severe hypotension,
sepsis or
vascular thrombosis(1, 14, 15, 49, 54). Reconstructing
the clinical course of events is made easier if one is aware of
the ABO compatibility and crossmatch status. Under ABO-compatible
circumstances, humoral rejection is most often confused with
"preservation"
injury and the pre-sensitization state and clinical profile can
provide information useful for the interpretation of the histopathologic
findings. For example, a recipient that harbors high titer (>
1:32-500) preformed IgG lymphocytotoxic anti-donor antibodies,
should be assumed to be at greater risk for humoral rejection,
compared to a recipient with low titer (< 1:32) anti-donor
antibodies. The diagnosis of humoral rejection is strengthened
when there is no obvious technical or other cause of allograft
dysfunction(23, 26, 40), and if there is persistence of the preformed
antibodies after transplantation. In addition, an antibody insult
is usually accompanied by a drop in the platelet count and persistent
thrombocytopenia below 50,000, and hypocomplementemia, as compared
to normal pretransplant values(40).
The clinical findings should be interpreted in conjunction with
histopathologic findings on liver biopsy. Histopathological clues
that humoral rejection may be occurring include arterial endothelial
cell hypertrophy, arterial medial thickening and myocyte vacuolization
associated with features suggestive of parenchymal ischemia, such
as centrilobular hepatocellular swelling or frank necrosis(1).
The more definite histopathologic features of humoral rejection,
such as lymphocytic arteritis and fibrinoid necrosis, are rarely
seen in a peripheral needle biopsy. With severe preservation injury
the cholangiolar proliferation, acute cholangiolitis, centrilobular
swelling and hepatocanalicular cholestasis generally improve over
time. These same changes generally worsen with time in patients
with humoral rejection, unless additional immunosuppression is
given.
Recently, a syndrome of fever and sudden deterioration of graft
function which mimics humoral rejection has been seen in association
with high levels of interferon- and tumor necrosis factor-, but
without preformed antibodies(55). Other groups have observed progressive
deterioration of allograft function associated with severe microvascular
steatosis on light microscopy that was could not be attributed
to a specific cause(56).
REFERENCES
Demetris AJ, Murase N, Nakamura K, et al. Immunopathology of
antibodies as effectors of orthotopic liver allograft rejection.
[Review]. Semin Liver Dis 1992;12(1):51-59.
Furuya T, Murase N, Nakamura K, et al. Preformed lymphocytotoxic antibodies:
the effects of class, titer and specificity on liver vs. heart
allografts. Hepatology 1992;16(6):1415-22.
Iwatsuki S, Iwaki Y, Kano T, al e. Successful liver transplantation
from crossmatch positive donors. Transplant Proc 1981;13(1):286-288.
Starzl TE, Ishikawa M, Putnam CW, et al. Progress in and deterrents
to orthotopic liver transplantation, with special reference to
survival, resistance to hyperacute rejection, and biliary duct
reconstruction. Transplant Proc1974;6:129-139.
Andres GA, Ansell ID, Halgrimson CG, et al. Immunopathologic studies of
orthotopic
human liver allografts. Lancet 1972;5:275-281.
Porter KA. Pathology of the orthotopic homograft and heterograft. In:
Starzl TE, ed. Experience in Hepatic Transplantation. Philadelphia:
W.B. Saunders, 1969:422-471.
Demetris AJ, Jaffe R, Starzl TE.
A review of adult and pediatric post-transplant liver pathology.
[Review]. Pathology Annu 1987;22:347-386.
Houssin D, Gugenheim B, Bellon B, et al. Absence of hyperacute rejection of
liver allografts
in hypersensitized rats. Transplant Proc 1985;17(1):293-295.
Houssin D, Bellon B, Brunaud MD, et al. Interactions between liver allografts
and lymphocytotoxic alloantibodies in inbred rats. Hepatology
1986;6(5):994-998.
Gugenheim J, Houssin D, Tamisier D, et al.
Spontaneous long-term survival of liver allografts in inbred rats.
Influence of hepatectomy of the recipient's own liver. Transplantation
1981;32(5):445-450.
Gugenheim J, Thai BL, Rouger P, et al. Relationship
between the liver and lymphocytotoxic alloantibodies in inbred
rats. Transplantation 1988;45(2):474-478.
Demetris AJ, Jaffe R, Tzakis
A, et al. Antibody-mediated rejection of human orthotopic liver
allografts. A study of liver transplantation across ABO blood
group barriers. Am J Pathol 1988;132(3):489-502.
Hubscher SG, Adams DH, Buckels JA, et al. Massive
haemorrhagic necrosis of the liver after liver transplantation.
J Clin Pathol 1989;42(4):360-370.
Gordon RD, Iwatsuki S, Esquivel CO, et al. Liver
transplantation across
ABO blood groups. Surgery 1986;100(2):342-348.
Rego J, Prevost F, Rumeau JL, et al. Hyperacute rejection after ABO
incompatible
orthotopic liver transplantation. Transplant Proc 1987;19(6):4589-4590.
Gugenheim J, Samuel D, Reynes M, et al. Liver transplantation
across ABO blood group barriers. Lancet 1990;336(8714):519-523.
Hanto DW, Snover DC, Sibley RK, et al. Hyperacute rejection of a human
orthotopic liver allograft in a presensitized recipient. Clin
Transpl 1987;1:304-310.
Starzl TE, Demetris AJ, Todo S. Evidence for hyperacute rejection of
human liver grafts:
The case of the canary kidneys. Clin Transplant 1989;3:37-45.
Takaya S, Duquesnoy R, Iwaki Y, et al. Positive crossmatch in
primary human liver allografts under cyclosporine or FK 506 therapy.
Transplant Proc 1991;23(1 Pt 1):396-399.
Karuppan S, Ericzon
BG, Moller E. Relevance of a positive crossmatch in liver transplantation.
Transpl Int 1991;4(1):18-25.
Takaya S, Bronsther O, Iwaki Y,
et al. The adverse impact on liver transplantation of using positive
cytotoxic crossmatch donors. Transplantation 1992;53(2):400-406.
Takaya S, Iwaki Y, Starzl TE. Liver transplantation in positive cytotoxic
crossmatch cases using FK506, high-dose steroids, and prostaglandin
E1. Transplantation 1992;54(5):927-929.
Moore SB, Wiesner RH, Perkins JD, et al. A positive lymphocyte
cross-match and major histocompatibility complex mismatching do
not predict early rejection of liver transplants in patients treated
with cyclosporine. Transplant Proc 1987;19(1 Pt 3):2390-2391.
Imagawa DK, Noguchi K, Iwaki Y, Busuttil RW. Hyperacute rejection
following ABO-compatible orthotopic liver transplantation--a case
report. Transplantation 1992;54(6):1114-1117.
Ogura K, Terasaki PI, Koyama H, et al. High
one-month liver
graft failure rates in flow cytometry crossmatch-positive recipients.
Clin Transplant 1994;8(2 Pt 1):111-115.
Lobo I, Spencer C, Douglas MT, et al. The lack of long-term
deterimental effects on liver allografts caused by donor-specific
anti-HLA antibodies. Transplantation 1993;55(5):1063-1066.
Donaldson PT, Thomson LJ, Heads A, et al. - IgG donor-specific crossmatches are not associated with graft rejection or poor graft survival after liver transplantation. An assessment by cytotoxicity and flow cytometry. Transplantation 1995;60(9):1016-1023.
Starzl TE, Valdivia LA, Murase N, et al. The biological basis of and
strategies for clinical xenotransplantation. Immunol Rev 1994;141:213-244.
Langer A, Valdivia LA, Murase N, et al. Humoral and cellular immunopathology
of hepatic and cardiac hamster-into-rat xenograft rejection. Marked
stimulation of IgM++bright/IgD+dull splenic B cells. Am J Pathol
1993;143(1):85-98.
Qian S, Fu F, Li Y, et al. - Presensitization
by skin grafting from major histocompatibility complex class I
or major histocompatibility complex class II deficient mice identifies
class I antigens as inducers of allosensitization. Immunology
1995;85(1):82-87.
Thai NL, Fu F, Qian S, et al. - Cytokine mRNA
profiles in mouse orthotopic liver transplantation. Graft rejection
is associated with augmented TH1 function. Transplantation 1995;59(2):274-281.
Manez R, Kelly RH, Kobayashi M, et al. - Immunoglobulin G lymphocytotoxic
antibodies in clinical liver transplantation: studies toward further
defining their significance. Hepatology 1995;21(5):1345-1352.
Gugenheim
J, Charptentier B, Gigou M, et al. Delayed rejection of heart allografts
after extracorporeal donor-specific liver hemoperfusion. Role of Kupffer cells. Transplantation
1988;45(3):628-632.
Gugenheim J, Houssin D, Emond J, et al. Delayed rejection of heart allografts in hypersensitized rats by extracorporeal donor-specific liver hemoperfusion. Transplantation
1986;41(3):398-400.
Nakamura K, Murase N, Becich MJ, et al. Liver
allograft rejection in sensitized recipients. Observations in
a clinically relevant small animal model. Am J Pathol 1993;142(5):1383-1391.
Astarcioglu I, Gugenheim J, Crafa F, et al.
- Hyperacute rejection of liver allografts in sensitized rats:
role of nonparenchymal liver cells. J Surg Res
1995;58(2):182-188.
Valdivia LA, Fung JJ, Demetris AJ, et al.
Donor species complement after liver xenotransplantation. The mechanism of protection from hyperacute rejection. Transplantation
1994;57(6):918-922.
Knechtle SJ, Kolbeck PC, Tsuchimoto S, et al. Hepatic transplantation into sensitized recipients. Demonstration of hyperacute rejection. Transplant Proc 1987;19(1 Pt 2):1082-1083.
Demetris AJ, Jaffe R, Tzakis A, et al. Antibody mediated rejection
of human liver allografts: transplantation across ABO blood group
barriers. Transplant Proc 1989;21(1 Pt 2):2217-20.
Woodle ES, Perdrizet GA, Brunt EM, et al. Reversal of humorally mediated
rejection following ABO-incompatible liver transplantation. Transplant
Proc 1991;23(6):2992-2993.
Sanchez-Urdazpal L, Sterioff S, Janes
C, et al. Increased bile duct complications in ABO incompatible
liver transplant recipients. Transplant Proc 1991;23(1 Pt 2): 1440-1441.
Weber T, Marino IR, Kang YG, et al. Intraoperative blood transfusions in highly alloimmunized
patients undergoing orthotopic liver transplantation. Transplantation
1989;47(5):797-801.
Batts KP, Moore SB, Perkins JD, et al. Influence of positive lymphocyte crosmatch
and HLA mismatching on vanishing bile duct syndrome in human liver
allografts. Transplantation 1988;45(2):376-379.
Gubernatis G, Kemnitz J, Bornscheuer A, et al. Potential various
appearances of hyperacute
rejection in human liver transplantation. Langenbecks Arch Chir
1989;374(4):240-244.
Burke GW, Cirocco R, Viciana A, et al. - Early graft loss secondary to
massive hemorrhagic necrosis following
orthotopic liver transplantation. Evidence for cytokine-mediated
univisceral Shwartzman reaction. Transplantation 1996;61(9):1370-1376.