|
Biopsy Evaluation of the Donor Organ Increased utilization of transplantation as treatment for patients with end-stage hepatic disease has resulted in a significant shortfall of available livers. Efforts to expand the available donor pool have resulted in the inclusion of older donors and others, who because of underlying chronic non-hepatic disease, might not have been considered in the past. This has resulted in more requests for frozen section biopsy evaluation of the liver and other organs from "marginal" donors. In conjunction with other data, the information gained from the biopsy analysis is used to determine whether the organ is suitable for transplantation (1, 2). If possible, the pathologist should grossly inspect the organ and assist in choosing the biopsy site and type. In general, a 1.5 cm2 subcapsular wedge or 2.0 cm long needle core from the anterior inferior edge of the liver is adequate in most cases, when the anticipated changes are diffuse. Biopsy sampling of the interface between the normal parenchyma and a mass lesion or focal defect is intuitive.
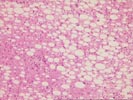
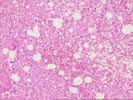
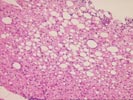
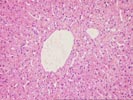
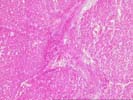
The donor liver is most frequently subjected to biopsy analysis. Frozen section requests are most often prompted by the macroscopic appearance of the organ, which raises uncertainties in the mind of the recipient surgeon. A grossly fatty liver most often prompts the request for biopsy evaluation. Currently, transplantation is contraindicated when a malignant tumor or severe macrovesicular steatosis , involving 60% or more of the parenchyma is detected(1-4). Donors livers with this degree of steatosis predictably cause a typical syndrome in the recipient shortly after reperfusion, which is caused by lysis of the steatotic hepatocytes .
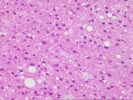
In livers with less severe macrovesicular steatosis , it is up to the recipient surgeon to decide when less than optimal organs are used for transplantation. They are best able to determine the risk to benefit ratio of using a particular organ for transplantation in a particular recipient. For example, donor livers with less than 30-40% macrovesicular steatosis will function after transplantation, but the recipient will suffer from fibrinolysis and a bleeding diathesis shortly after reperfusion. Microvesicular steatosis on the other hand, is often found after a short period of warm ischemia and other insults. In our experience, it usually does not predictably result in post-transplant graft dysfunction and therefore, is not a contraindication to transplantation. In other instances, a mass lesion or even the clinical circumstances surrounding the donor's death may trigger the need for quick histopathologic evaluation of the graft.
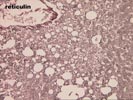
In our experience, the routine H & E stained frozen section are adequate to determine the severity of steatosis; fat stains are not necessary. There are however, several important caveats that deserve particular mention. It is extremely important that the biopsy is freshly obtained. Fat quickly leeches from liver biopsies left open to the ambient air or resting on a dry paper towel for more than several minutes. In such cases, a subsequent frozen section can significantly underestimate the severity of steatosis. Organs that otherwise would have been discarded will be used, often with disastrous consequences. In addition, biopsies kept in "physiological" saline are significantly distorted by this medium, such that interepretation becomes extremely difficult, if not impossible. Clumping of the cytoplasm and edema of the extracellular spaces distorts the morphology so much so, that it becomes impossible to detect areas of necrosis.
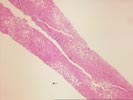
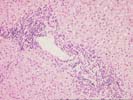
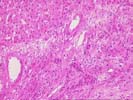
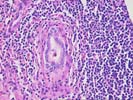
Predominantly mononuclear portal inflammation is a common finding in donor organ biopsies. In such cases, the differential diagnosis is quite broad, because the findings are usually mild and non-specific. Viral hepatitis infection, particularly type C, should be excluded in such cases. The serological test results for hepatitis infection are usually available from the procurement agency and known to the donor surgeon. In the absence of viral hepatitis infection, a prolonged stay for more than two to three days in the intensive care unit for the donor is commonly associated with this finding. In such cases, the liver can be used without any problems.
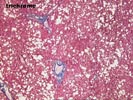
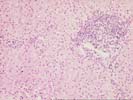
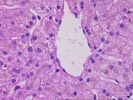
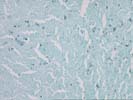
Several frozen sections have been requested from inexperienced donor surgeons, because the liver has "a funny color", which is usually greyish-brown. In most instances, such requests can be handled over the telephone, without a frozen section by simply asking the donor's age. However, a persistent surgeon may still request that the liver be examined microscopically. In such cases, lipofuschin , which is deposited primarily in the centrilobular regions is responsible for the gross coloration. It increases with age, such that donors older than 60 years will contain enough lipofuschin to grossly affect the color of the liver. Inexperienced pathologists can mistake lipofuschin pigment for cholestasis or iron deposits. Iron deposits in the early stages of genetic hemochromatosis are periportal, in contrast to the centrilobular predominance of lipofuschin. Bile stasis can be distinguished from lipofuschin by the presence of pigment in the canaliculi, between the hepatocytes and bile is amorphous, whereas lipofuschin is more granular in appearance.
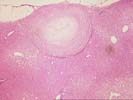
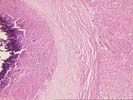
Focal nodular hyperplasia(FNH) lesions are occasionally detected on frozen section of donor livers. Most often, these are detected on frozen section evaluation of small(1.0 - 3.0 cm) subcapsular nodule(s). Another name for FNH is "focal cirrhosis". Remembering this name is helpful in making the diagnosis. This older name also should serve as a reminder that the pathologist has to be aware that the donor liver is being evaluated for a focal lesion, so a mistaken diagnosis of cirrhosis is not made.
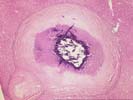
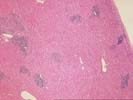
Small firm white, well-circumscribed subcapsular nodules also frequently prompt a request for frozen section evaluation of the donor liver to rule out a primary or metastatic malignacy. Often, these turn out to be old fibrotic granulomas from histoplasmosis, or "histoplasmomas" .
Non-central nervous system malignancies are a contra-indication to liver transplantation. When such lesions are encountered, the donor organ is disgarded or used for research purposes. It may be difficult however, in some cases to make a diagnosis of a neoplasm with certainty, particularly on frozen section. This is particularly true for hematolymphoid tumors , which are notoriously difficult to diagnose in this circunstance. It is best in such cases to err on the conservative side, particularly if the potential recipient is stable enough to wait for another donor. In addition, in many cases it is particularly helpful to examine any other donor tissue that might provide useful information. REFERENCES
Please mail comments, corrections or suggestions to the TPIS administration at the UPMC.
If you have more questions, you can always email TPIS Administration. |
||||